Something that is not much talked about is the fact that many people apparently die from a sepsis (bacterial) that is caused by the primary infection.
In Italy, it is almost customary to pop medication that contains antibiotics whenever you feel a bit under the weather. I lived in Italy, I experienced this first hand even from my more educated friends.
Because of this Italians have an antibiotics resistance of 26.8% [1].
I do not have data for South Korea but in Germany, where I live, antibiotics are not available over the counter. You always need to see a professional and then they are much more expensive that e.g. in Italy.
The resistance rate here in Germany is 0.4% [1]. That's 67 times (!) lower than in Italy.
This is fascinating, I didn't know that data about antibiotic resistance was available like this, and definitely had no idea there was such huge variation between countries.
Surely this should be considered a major public health emergency in itself?
Are the countries with high percentages taking steps to limit antibiotic use? Coming from the UK the idea of letting people buy antibiotics as easily as painkillers seems crazy.
> Surely this should be considered a major public health emergency in itself?
Indeed. There's an episode of Sam Harris's podcast with Matt MCarthy from last summer. The episode title is The Plague Years, and they go into quite a bit of detail on this sort of thing and ruminate about how low on the radar it is for most people (if it even registers at all), despite the seriousness of the situation.
A large number of South Korea infections are even younger due to how it spread.
Another possibility is that Italy doesn't have a handle on who is or isn't infected so what they report are the obvious infections, who tend to be older.
>Another possibility is that Italy doesn't have a handle on who is or isn't infected so what they report are the obvious infections, who tend to be older.
This is very likely the case, as can be seen in the positive test outcome rates.
16.7% in Italy vs. 3.6% in South Korea
Italy has run around 60k tests.
South Korea are testing around 15k people/day and have tested 234k people in total. They've even setup drive-through testing centers where anyone can drive through, get tested, and get results via SMS in under a day.
The result of this is likely a much larger number of asymptomatic or mild cases in the South Korean numbers, which based on the China data, tend to be a lot younger.
Yup. Meanwhile, the New York Times has run an article about how northern Italy is "a warning to the world" with the eye-catching claim that "about 50 percent of the people who tested positive for the virus required some form of hospitalization": https://www.nytimes.com/2020/03/12/world/europe/12italy-coro... Between this and other reporting, I'm starting to wish they hadn't opened up their paywall for coronavirus articles.
Yes, not only in Italy, but in most other places. This article explains well how deaths (or hospitalizations) are correlated to actual infections (most of which go unnoticed), and also why reduction of social interaction is effective but its effects take a while to show:
In many (technically former) "red zones", especially in Lombardy, they tested also asyntomatic family members of infected people, or their contacts. I'm not sure how inaccurate it is, but I have no idea what has been done in SK.
South Korea traces the movement of everyone who tests positive, puts the movements online and tests those who were exposed to someone positive (this is in the article I believe). It's a massive effort but with the world economy at a stand-still, what else do people have to do?
North Italy has a population of 27 people btw so the 10K that are registered as positive as a drop in the bucket.
It is possible you are right. IIRC, 17% of those tested were positive in Italy. That's a very high percentage. Very likely the actual infected number is much higher.
Yup, you probably only have to look at the counts of infected tourists coming back. In Norway that is 89 from Italy, and 112 from Austria (25% of the total infected as of writing...)
True, same here, in The Netherlands. Of the first 500 reported cases, around 25% were tourists returning from the Alps region (northern Italy, western Austria), and around 50% were traced to secondary infections from those first 25%. The other 25% were unexplained, hence we're now in the endemic spread phase.
FAFAIK, we've never had a policy to pre-emptively test every returning tourist, and even now we don't test everybody. The current policy is to test new cases only if they have no relation to an already-established case. For example, people living in the same house as a known Corona case will not get tested. If they start showing symptoms, they're automatically assumed to have contracted it.
No. In fact they just revised their testing criteria and will not test most people who are asked to quarantine at home. Testing is expected for people who have acute respiratory illness, people who are hospitalized, health care workers handling these cases, and immune-compromised people with mild symptoms.
It’s unlikely that 14,000 infected 20-29 year olds where missed as a significant fraction end up in the ICU. Which means even if the ratio is off, the breakdowns are still significantly different.
I'm not sure how the media should report on deaths over 80, or even over 90.
It's not that old people aren't worthy of protection, but when you're 85 in the US you have a 10% chance of dying in the next year for any and all reasons.
So saying this disease kills 15% (for example) of 80+ year olds without context sounds horrific, but contextualized in the actual risks of just being very old to begin with, sounds much less scary.
If Italy, for example, were to report on the number of fatal infections in people younger than the natural life expectancy, the fatality rate would drop in half.
Fatality numbers won't reflect those who developed permanent lung damage or had to go into intensive care.
Best not to suggest anything that might down play the seriousness considering how infectious this virus is. (Otherwise it may encourage risky behavior.)
I think it's best not to overstate like the media currently has been (at least here in the USA) which is that everyone should be panicky and worried if they'll be alive next week.
It's far too early to draw any conclusions, but the HK Hospital Authority has suggested that they are seeing reduced lung function in some "recovered" patients.
but what about the risks of over-selling this disease? Look at Italy for example. I've read self-reports from healthcare workers claiming 200% hospital capacity. I can only image the needless death resulting from such panic.
Mind you that isn't covid 19 putting them over-capacity. In the worst hit region in Italy (Lombardy) confirmed covid 19 cases represent enough cases to take up less than 10% of their hospital beds. So it seems incredibly unlikely anything but panic is to blame for such absurdly high over capacity.
> Giulio Gallera, Lombardy’s health chief, said Thursday that the region would reach its capacity in “five, six or seven days,” even if it tried to add more beds in hospital “cellars.” In an interview with Italy’s La7 channel, Gallera described the possibility of adding 500 intensive-care beds at Milan’s expo center, the kind of rapidly assembled zone that China created in the hard-hit Wuhan area.
lombardy has 7280 confirmed cases [1]
lombary has a population of 10MM (wikipedia)
italy has 3.18 hospital beds per 1000 [2]
the math for that adds up to 31,800 hospital beds
7280 confirmed cases is 22% - so my sources were off or wiki is wrong as originally I recall reading lombardy has a 16MM population.
I will say that your article claims they haven't run out of ICU beds yet but that number is surprisingly high for ICU needs to cover covid 19. The article implies 600 ICU cases from covid 19 - that's over 12% ICU from confirmed covid 19 cases, which is more than twice what china reported.
It's also very surprising how few ICU beds they have allocated towards ICU....
The USA has something like 14% of hospital beds as ICU beds [3] but Italy appears to only have have less than 3% of their beds available for covid 19 ICU
Most hospitals don't have all that much slack in bed capacity; especially at the tail end of flu season most of those beds are already filled. The hospitals may be extrapolating the growth rate of the disease and realizing how soon they will have problems. Or given the nature of the outbreak it could be that even within Lombardy there are areas with much higher concentrations of cases, like there are more cases, inc. per capita, in Wuhan than other cities in Hubei.
What's not plausible is ICU beds being taken up by people who don't have the disease (maybe miild-to-moderate flus or bad colds) and are just panicking. Emergency room lines, sure. Test shortages, absolutely. But hospitals will not put someone who's just scared and doesn't even need to be admitted at all into the ICU.
> Most hospitals don't have all that much slack in bed capacity; especially at the tail end of flu season
Remember that there's a difference between hospital beds and ICU beds.
In the UK, we maintain 80% utilisation of our ICU beds all year round[0], with very little change in the number of beds available in real number terms. We have ~4100 total ICU beds, which can be expanded to ~5000 if all operating theatres, etc are shut down and used as ICU equivalent instead.
While getting past flu season will help the total number of beds, it does nothing for the ICU.
This is the other reason why it's increasingly important to https://www.FlattenThesCurve.com and employ social distancing techniques. The rate of patients being admitted into ICUs needs to be slowed as much as possible. Once we're out of capacity, every additional patient has a much higher probability of dying than the overall fatality statistics indicate.
The NHS regularly has to cancel routine operations in order to free up space for flu patients during the flu season, which might be one reason why the bed usage seems so uniform. Obviously if they're already doing that for flu it leaves less slack in the system if something else comes along.
1. Not every hospital bed is the same as a bed for a highly infectious disease
2. Other things still happen to people and those people need to have their hospital beds.
3. I'm not a hospital planner but I think there may be other things that determine capacity than just hospital beds. I worry that the hospital bed metric is actually a bad metric. Obviously adding hospital beds implies adding people to staff those beds, but also adding people probably also means adding all sorts of other infrastructure to support those people.
As a developer it reminds me of a project that goes way off schedule, you don't bring the project back on track just by adding developers because of the overhead more developers add to your system. Probably most hospital administrators have never actually experienced operating at capacity, so estimations of what would happen could be off and are being corrected now.
Maybe you shouldn't transfer every confirmed case into hospital since most cases will do just well ... unless they don't. (Not questioning the danger of this virus.)
Your 10% premise is wrong because you're conflating intensive care capacity and regular hospital beds. You can't just put Covid patients in with the general hospital population and it isn't trivial to convert other hospital beds to the requirements of Covid while ensuring you keep everyone else in the hospital safe from infection. Lombardy does not have anywhere near enough intensive care capacity to handle the cases they've already seen, much less anything further.
You can see that in the death rate, it's happening because they can't care for the volume of older intensive care patients properly. They don't have the medical infrastructure capacity to do it. That's why Italy and other European nations such as France have an extreme variance in mortality rates, despite France and Italy both having similarly old populations. Germany is even older than Italy and I'm skeptical we're going to see anywhere near a 6% mortality rate there (their rate is very low so far). Italy's mortality rate has been abnormally high from the first few thousand cases in, when it quickly began overloading their healthcare system in Lombardy.
A quick google suggests around 15% of hospital beds are ICU and covid 19 cases that end up in the hospital, only 5% end up in ICU. So that's an interesting line of thinking but it lacks supporting evidence that covid 19 is overwhelming ICU.
edit to address your edit: The mortality rate is often wildly inflated with new diseases. That's because most people don't seem to understand real mortality rate vs confirmed cases mortality rate. Obviously when a disease is new the confirmed cases will be confirmed against the people showing serious symptoms. Then when you pretend deaths/confirmed cases == mortality rate you end up with a wildly inflated mortality rate. Until we understand how many people are asymptomatic we won't have a real mortality rate that is reliable.
Percentage of ICU beds varies widely. Minnesota, for instance, a state in the US, has about 500 ICU beds [1] and over 10,000 hospital beds total [2]. ICU beds are already heavily used and sometimes there simply are not enough, before COVID-19 has even shown up. Average inpatient stays right now are 4.21 days in Minnesota [3]; I can't find a reliable number for length of stay for COVID-19 patients, but it is longer.
There is plenty of evidence that in Italy COVID-19 has overwhelmed ICU beds. They are trying to transport people to ventilators via helicopter. We do have at least twice the ICU bed capacity in the US (compare info from [4], [5]). But many other people need these ICU beds -- it's not like other illnesses will just stop for our convenience.
The ICU beds are also taken by all the other sick people. Only a minority is actually free. And people don’t end up in the ICU because they panic:
I spoke to several Italian hospital doctors and they are overwhelmed by the troves of patients who can’tbreathe.
Right: we do have those ICU beds because people are in them.
Toolz, I just don't understand your math. You seem to assume that a neonatal ICU bed is just as good for a 55-year-old man as an adult one, and that no one is going to have any other ICU-needing illnesses for the duration of this epidemic. That's quite puzzling. Can you support these ideas?
I just read an article that claimed Lombardy has 737 ICU beds available for covid 19. Given Italy has a 3.18 beds per 1000 people that means they have less than 3% of their hospital beds available for covid 19 patients. That's absurd. In relation the USA has roughly 14% of their beds as ICU beds according to a reference from https://www.sccm.org/Communications/Critical-Care-Statistics
You seem to think that for some reason, ICU beds go unused except in a situation like this? ICU capacity is probably built to meet some fraction of demand in normal circumstances. Those beds weren't all unused before this outbreak started.
737 ICU beds available isn't the same as the total number of ICU beds. Normal health problems that need hospital treatment (strokes, heart attacks, car accidents, etc.) are still happening during this outbreak (well, car accidents are probably reduced now with Italy's lockdown protocols).
Hospitals worldwide have very little spare capacity and even less spare ICU capacity. A normal hospital bed isn’t going to help much. They are very likely to be overwhelmed, especially in countries that have not been able to delay initial spread due to lack of testing and containment.
This probably won’t kill millions (though it could worst case) but hospitals being overwhelmed would lead to an exponential rise in deaths, and many deaths from other causes as other treatments are abandoned. The situation is serious and will require significant measures to bring it under control, it is not yet being taken seriously enough in the US.
When you have ADRS ICU treatement is pretty much the only thing keeping you alive. "Randomized trial" in this context means russian roulette - if you don't get a ventilator you'll die almost certainly.
Evidence [0] (partly based on COVID-19, parly on MERS) also says that NIV has a significantly worse outcome than ventilation. People are already getting NIV in some hospitals because they ran out of tubed ventilators.
An additional factor in why the death rate is so high in >75 year olds is that most deaths happen when ICUs are overwhelmed, and older ages get triaged into not getting a ventilator. There is a much higher rate for them naturally, but this amplifies the disparity even more.
That's a really hard thing to say this early. For all we know many 80+ people are asymptomatic and most older people aren't negatively affected at all by covid 19. It seems really dangerous to conflate actual mortality rate with mortality rate among the confirmed cases. Those numbers will be drastically different with diseases that have many asymptomatic carriers.
I'm surprised to hear someone be so blunt about their ageism. This thing has brought about a great deal of it already, with many saying, " it only affects the elderly" as if that's a worthwhile argument for not being too worried. Reminds one of indifference to AIDS in the 80s because it "only affects homosexuals"
> It's not that old people aren't worthy of protection, but when you're 85 in the US you have a 10% chance of dying in the next year for any and all reasons.
Some of the people that die from this would have died anyway, but for the most part this is on top of that 10% chance. Same for young people, there's something like a 0.2 chance of death every year and this is basically doubling that.
The numbers for 20-29 are probably not comparable. South Korea has been testing a lot of people per day. Italy, like many other countries, is overwhelmed, so there are probably many healthy-feeling infected 20-somethings who haven't been tested and aren't counted.
If you factor in collapse of medical services -- Italy ran out of ventilators / ICU beds--the gap becomes clearer. You have to look at over 60 as more likely to be hospitalized, putting strain on medical system.
This doesn’t account for it because South Korea didn’t even have the number of serious cases that Italy has.
The real answer is simply that the number of tests is not equal to the number of cases.
The number of positive tests is a factor of the number of tests done, and how selective the testing was allowed to be. It is only loosely related to the number of infected people (technically it is the lower bound).
My comment was directed at age structure of population accounting for difference in mortality, complicated by effective collapse of medical care in certain regions of Italy that meant severe cases that could have been managed because critical and then fatal without ventilation support.
Speaking to Euronews on the condition of anonymity, she said: "We have hundreds of cases in our hospital. Half of our operating block has been dedicated to COVID-19 patients. The situation is dire. Anesthetists – despite them playing it down a little bit on the media – have to choose who they attach to the machine for ventilation, and who they won’t attach to the machines"
---
A first person report from Seattle ICU doctor https://www.facebook.com/marie.e.will/posts/1016307125424515... "Remdesivir might work, some hosps have seen improvement with it quite rapidly, marked improvement in 1-3 days. ARDS trajectory is impressive with it, pts improve much more rapidly than expected in usual ARDS. Recommended course is 10d, but due to scarcity all hosps have stopped it when pt clinically out of the woods - none have continued >5d.
I decode this as they have half the amount of Remdesivir they need, only treating for 5 days when recommended course is 10.
The other thing that appears to be going on, and it's also hinted at in report from Seattle, is that old patients are being moved to hospice or "comfort care" who would not have been three months ago because of lack of supplies/personnel/equipment.
#1 provides no numbers and no details beyond a claim that "They lack machines to ventilate all those gasping for air."
#2 does not even go that far: it speaks of "a huge turnover issue and leaving hospitals at near capacity" (near, not above, contradicting #1)
#3 is from an intensivist in Seattle, Washington, not from Italy.
I chose the Washington Post link because it provides numbers: "Lombardy has just 737 intensive-care beds available for coronavirus patients. More than 600 are filled. [...] The region is racing to bring more beds online; it added 127 on Thursday."
(Lombardy is the region with most cases.)
This is consistent with the claim in your link #2 that hospitals are near capacity (and not above it, as suggested by your link #1).
The point of all this pedantry is simply that I don't think saturation can be invoked yet to explain the high Italian mortality rate.
Addition:
Here's a slightly older Italian source (March 11) which puts nation-wide ICU capacity in Italy at 5090, with 887 in use:
#3 was to show what can happen in one hospital. These patients are hard to transfer. Lombardy is about 9200 sq mi. (about 100 miles square). If you need a ventilator you may not be able to withstand a 50 mile ambulance ride. But I concede I cannot offer conclusive proof that Italy is out of ventilators.
from the translation it does not appear they are moving Covid-19 patients: "For the first time, Lombard hospitals have had to resort to the Remote Health Relief Operations Center (CROSS), which intervenes when a region is no longer able to cope with the number of patients and must seek help from other regions. The Civil Protection has ordered that a number of ICU patients in Lombardy for other diseases be transferred to hospitals in neighboring regions."
Note this is first time it's been triggered which indicates it's a difficult and risky process.
Article also notes "The people in charge of intensive care in Lombardy have sent a dramatic appeal to Governor Attilio Fontana: "Healthcare facilities are under greater pressure than any possibility of adequate response", the doctors write. "Despite the enormous commitment of all healthcare personnel and the deployment of all available tools, correct management of the phenomenon is now impossible."
This sounds like a system that's out of ICU beds.
see also https://jamanetwork.com/journals/jama/fullarticle/2763188 "As of March 8, critically ill patients (initially COVID-19–negative patients) have been transferred to receptive ICUs outside the region via a national coordinating emergency office."
> Speaking to Euronews on the condition of anonymity
This should imply heavy fines. Creating panic while covered by anonymity is very easy and it brings no value to society. If officials later on try to bring real numbers nobody listens.
The infection in Italy started in hospital or in retirement home (I don't remember which), so the first infected were people > 70.
In South Korea it started in a cult, where most people were young < 40, and moslty women (which have less CFR than man for COVID-19).
And the rest was South Korean lack of regard for privacy (they have a map for each case where you can trace where and when a given infected person was - so you can check if you were near him/her) and technological superiority.
I don't know what their age profile is, but the outbreak began with a 61-year old ("Patient 31"), and several people mentioned here are above 50 (the founder is 88):
About 80% of South Korean cases were less than 60 years old, with a peak in the 20s [1]. It is widely rumored that Shincheonji prefers to recruit young people who are easier to exploit.
My guess is that there are a lot of unreported cases in Italy while in Korea authorities seem to ran more vigorously tests. So the latter might have much more accurate numbers than the former.
You say "rigorous tests" OP said "vigorously tests". Very different meaning. The test in both countries is essentially the same, and thus the same rigor (in terms of sensitivity and specificity). The vigor by which the testing was performed (in terms of #people tested as a % of total pop) is WAY WAY higher in S. Korea.
South Korea used to be at about the same development index as Italy maybe...20 years ago? Today it's tied with Israel (as of 2018) and above Spain, France, and Italy.
The PPP is also about 10% higher than Italy and has about half the unemployment rate.
Yeah, I also heard that China is sending to Italy the materials they don't need anymore, since they started dismantling the temporary hospitals in Wuhan. That would be very helpful.
It's also easier to leave Italy and spread the disease because it doesn't have a DMZ in the North and lots of migrant workers and other EU nationals, free to leave at any time. Some have fled the lockdown using ferries through Croatia or Greece and then on to their home countries. When the North was quarantined, many Italians irresponsibly fled to the South, prompting the authorities to issue a country wide lockdown. Good luck trying to escape by ferry from Korea to Japan, Russia or China in the middle of a pandemic. North Korea is out of the question. Also Koreans are likely to obey the rules imposed during a healty emergency crisis (they also has a MERS epidemic in 2015), while Italians are more likely dismiss them as nonsense.
Except if the increased rate of death is from the medical system being over capacity.... this still wouldn't be a good test of quality of their responses, but more just revealing the capacity of their medical system.
Please don't conflate case fatality rate with actual fatality rate. South Korea has almost certainly just had more time and "medical bandwidth" to find more of the minor and asymptomatic infections that make up potentially 80%+ of the total, and turn them into cases by diagnosing them.
I thought that actual fatality rate is always higher than measured in case of exponentially growing pandemics. Just imagine the case where it takes 20 days for people to die. Your calculations of fatality rate this early in the disease would be conservative.
A far bigger factor in a disease like this, where 80%+ of people have mild illness, is all the people that were never recorded as cases because their symptoms were too mild or were non-existent.
People want to use CFR as a measure of how worried they should be, or as some kind of comparison between countries, and it's totally inappropriate for either purpose.
If they are never recorded does that not mean they infect more people and that results in sicker population creating more burden to the health system - resulting in more deaths?
The statistics always seem to go up no matter what kind of interpretation.
The point is that deaths - the numerator of the case fatality rate - are basically always recorded, whereas cases - the denominator of the case fatality rate - represent only a subset of the people that are infected.
When the health system is severely overburdened, that subset because a smaller and smaller proportion, as scarce resources are used for testing of people presenting at hospitals rather than population-based testing.
People who are asymptomatic or have minor symptoms don't present at a hospital, so they don't get tested, so they never get recorded as a case (which, by definition, requires a test and a diagnosis).
The real population fatality rates are guaranteed to be lower than the CFR unless you believe that every person who is infected is being tested and diagnosed, and it's my opinion that they'll be much lower.
There are also cultural differences, Italians like to hang out in groups, outside, personal space is much smaller, people hug and kiss and touch all the time. Also they're not really the most disciplined nation, lots of them simply ignored the safety rules, continued to go out, there were even some cases where infected people run away from quarantine.
And additionally the spread of virus is not uniform as it depends on social circles, so it's very hard to compare the situations using just general population stats. In South Korea one of the early patients infected more than a thousand other people, while some patients infected no one else or only a few. It's totally random event, and a few patients like that can create a huge differences in the spread of the disease. In Italy they've had the bad luck that early on virus got into hospitals and retirement homes, so the most sensitive population was massively affected.
I think there is another factor as well: have a look at train stations during rush hour on East Asia currently vs. Europe. 1) the density is significantly higher but 2) nearly everyone is wearing surgical masks now. I think that mask wearing is an effective measure to slow down the spread, acting at the sender side rather than the receiver (which Western people tend to focus on). You can see a similarly lower exponential spread in other Asian nations compared to Europe and I think that masks plus a lesser degree of body contact can explain this largely.
Part of the problem is that pretty much everybody in East Asia already owned at least one mask.
In Europe pretty much nobody owned a mask prior to COVID-19. And masks have been sold out for weeks. If masks were easily available you'd see people wearing them I'm sure.
This is partly an effect of cultural issues related to immunity and how it's perceived in most europe countries.
Even putting aside the whole deliberate sharing germs and force building body resistance, wearing a mask is seen as anti-social, somewhat selfish, weak and alarming.
People's reactions to a mask is really ranging from "you shouldn't wear it at all, we're among friends (at work)" to "if you're that ill you shouldn't get out of your home and take a sick leave". There few middle ground, accepting wearing a mask just in a case, or for some benign infection.
At least in The Netherlands there are still plenty of masks to be found. You won't find the surgical masks anymore but masks for construction work is still plenty available.
I think most europeans look down on wearing masks as something stupid, most europeans also think hand sanitizer is stupid. (This just applies to my dutch family and friends over there, I am currently in Thailand and always wearing a mask and hand sanitizer)
Except no one seems to wear them fully correctly, and a lot of people don't have the proper rating of mask. Not to mention theres a limited supply of masks.
The part of Italy hit also has air quality, per aqi searches, that is comparable to the region in China that was hit hard.
Have people looked that it is not age, but baseline damage to your lungs that is the main factor in serious cases? Older people will have more exposure to local air pollution, just from having lived longer. That existing damage can be what contributes to complications, right?
Source? Right now air in Wuhan [0] seems to be significantly worse than Milan [1]. Both cities are under some level of quarantine, but it has been stricter and going on for much longer in Wuhan. Chinese sources say that the air in Wuhan is much better than it was before the quarantine. We can assume that the difference between the two cities would be even larger during normal activity.
Edit: Milan is much closer to Seoul [2] than to Wuhan.
I used those sites and looked at daily historical. I grant that China was strictly worse. But Milan is strictly worse than everywhere else getting hit.
Edit: and the air being better after the quarantine would support my hypothesis. It wasn't that that helped, but the better air. (Which is still very bad)
For reference, this is the site I found that went back farther. Milan is not constant days of 150, as Hubei is. That said, it is littered with many high value days. Contrasted with Seattle, which has been steady below 60 for the time period.
Take this over to Australia [below], and you can see that even they had terrible air as recently as mid January.
Contrast to Norway [also below], which has hovered on fine air quality for the entire time. Same for Japan, all told.
Basically, the worse your air quality, the more severe cases you are seeing. To a marked degree.
Edit: Just eyeballing, Milan is worse than Seoul. Agreed not as bad as Hubei. But between.
No, the far more likely explanation is that the total number of cases reported for Italy don't reflect reality.
Because they are overwhelmed Italian hospitals basically send people home if they have a fever or other symptoms with no test administered, instructed to come back in case the symptoms worsen, only people having trouble breathing being admitted in the ICU.
Italy could easily have in reality 10 times the number of reported total cases or more.
> Because they are overwhelmed Italian hospitals basically send people home if they have a fever or other symptoms with no test administered,
Sources, please.
> only people having trouble breathing being admitted in the ICU.
Well, why would you put someone without respiratory failure in an ICU to egin with?
Also, Italy performs 1 test per 1000 people [1]. Surely there are more cases than the reported ones, but 10 times? I am no statistician, but wouldn't it require extreme bad luck to miss so many cases with such extensive testing?
As posted else thread, the percentage of positive tests in Italy is almost 5 times larger than in Korea. This probably means that the infected population is much higher than what's being reported.
In the initial weeks of the crisis, the Italian government said that they would switch to only reporting symptomatic cases [1] ("because that what every body else is doing") instead of all positive tests. I do not know if they followed through, but that would make a large difference if Korea was reporting everything.
edit: as far as I understand, that only changes what they report in the official numbers that make the news. The actual medical data might contain the real numbers.
edit2: if they started doing what they said they would, the actual positive rate would be even higher. So the issue is likely that they are just not testing as much.
> This probably means that the infected population is much higher than what's being reported.
Agree, is the logical thing. The bigger the sample, the better the results.
Another possible option could be that caucasian people is more susceptible for some reasons than asian people. The reasons could be genetic or cultural (i.e previous exposition to similar viruses by gastronomy). Without more data, I would take the first option as closer to truth.
Did they test random people or only people with symptoms? If the latter then your distribution is heavily biased and a 10x difference is not an outlier, it's the expected outcome.
According to those stats 14% of people tested were positive and of those, about half had to be admitted to hospital. It's clearly very far from a random sample.
Also keep in mind that the false negatives for the tests is pretty high, because the tests require a significant viral load in the blood and in some cases it can take several days after the symptoms set in.
Just look at how many people from other other countries got infected in northern Italy a few weeks ago. Italy had diagnosed a few hundred cases, yet suddenly hundreds and hundreds of people who were in the area and have returned home now have it in other countries. It's clearly far more highly prevalent than testing suggests.
Yeah, but they've also been able to significantly slow the spread, growing at what looks to be closer to 10% day-over-day (doubling every week). Most everywhere else is seeing 25-35% (doubling every 2-3 days).
These go hand in hand. In the US we cannot slow the spread because we refuse to test anyone who doesn't need acute care or who doesn't have documented contact with travelers or foreign nationals. The research from Helen Chu's lab at University of Washington shows that this means we missed the start of community transmission entirely in Washington.
Here, there are health care workers who can't get a test! They deal with people with significant health problems every day and could be spreading it all over -- but because they didn't travel, they can't get a test.
New cases in SK are on a downward trend for around 10 days now. They achieved a reproduction value that is quite a bit below for at least the last 3 weeks.
I can understand how it is more susceptible to death but I don't see the connection with spreading. Old people tend to move about much less and none of the references support that older people are in any way more responsible for spreading the virus.
I think much better explanation would be that Italy has a lot of tourism, it is basically a tourism hub for northern and eastern Europe. Tourism == a lot of people moving about, very frequently, then leaving the country. Almost all initial cases here in Poland seem to be connected with somebody coming back from vacation in Italy.
More susceptible to deaths I understand, but is an older population more susceptible to spreading of the virus? Is probability of "infection given exposure" (as opposed to being a carrier) also greater with age? (I know that's true for kids, but hadn't heard if that trend continues across all age ranges.)
> South Korea has since reported 67 deaths out of nearly 8,000 confirmed cases, after testing more than 222,000 people. In contrast, Italy has had 1,016 deaths and identified more than 15,000 cases after carrying out more than 73,000 tests on an unspecified number of people.
Surely the testing is a huge factor. Test more people you'll find more people infected, so the fatality rate will get smaller. If you're like the US and test very few you get the huge fatality rates we saw in Washington.
If you could quickly and accurately test everyone in the country today we would know how to isolate and the whole thing would be over very soon. Not having a reliable test makes this whole problem as bad as it is.
Also, as an American, I'm embarrassed by my country's response and by how my president addresses the nation. PM Lee shows how you talk to your country:
Singapore has been competent, but Taiwan's response has been more impressive.
It's very close to the hot zone, millions of people travel to and from mainland China every year, it has roughly the population of Australia living on 10% of the land Japan has, the WHO refuses any cooperation, and yet there have been under 50 cases and no local transmission.
Not only that, but as a democratic state, Taiwan's control measures have been remarkably measured.
I'd credit two factors:
1) Imposing travel limits three weeks before China even admitted there was an outbreak. After SARS, the TW government had a plan for this epidemic and a healthy skepticism for both official news and the WHO.
2) Taiwan has a relatively high trust society. People generally trust the local CDC and make a genuine effort to take preventative measures, even those primarily for the safety of others. A phone alert is generally all that's needed as a quarantine reminder for those exposed.
> After SARS, the TW government had a plan for this epidemic and a healthy skepticism for both official news and the WHO.
That's not surprising, since the WHO doesn't recognise Taiwan as an independent country and refuses to help them, I'm glad they were able to take their own successful measurements.
Romania, which is also severely underprepared for a real outbreak. At least they're locking down borders and checking people, there's a lot of them going to/from work around the EU.
JAMA article about Taiwan - they made changes after SARS to have a faster response and what they did worked to contain the spread even though there is a large flow of people to/from China.
https://jamanetwork.com/journals/jama/fullarticle/2762689
Being a small country definitely helps in situation like this, it is not likely US as a big country can be as effective as Singapore. What do you want the government to do? lock down cities with troops?
For all those interested in how Singapore can possibly be a duality of "sometimes good sometimes bad", just look at how Singapore treats its Malay population as second class citizens.
For example, if a Singaporean Malay marries a Malaysian Malay, there is still a large chance their Permanent Residency application will be denied. This usually doesn't happen to someone who marries Han Chinese, of which Singapore is 70%.
Edit: If you're saying that the "reported" death rate "appears" lower based on reported statistics, then yes testing more people can make it seem like the actual death rate is lower. Otherwise:
> 67 deaths out of nearly 8,000 cases
> 1,016 deaths and identified more than 15,000
> Surely the testing is a huge factor.
No, you can not be sure at all, especially since it is well-known that hospitals have limited capacity to treat pneumonia (ventilators and doctors trained to use them). Get sick when hospital has no capacity to treat you, and you're more likely to die. Death rate will increase very rapidly when rates of infection pass a certain point.
Testing is important, yes, but the real important part is slowing the transmission rate to a manageable level.
> If you could quickly and accurately test everyone in the country today we would know how to isolate and the whole thing would be over very soon.
Only if you can do it more-or-less completely. Otherwise, you're actually prolonging the problem. The reason we want to slow the transmission of the virus is to keep life-threatening cases at a reasonably low rate.
Surely the testing is a huge factor. Test more people you'll find more people infected, so the fatality rate will get smaller. If you're like the US and test very few you get the huge fatality rates we saw in Washington.
Uh, yes, South Korea testing lots of people shows the overall fatality rate given a functioning medical system. It also allows much better isolation, understanding of the progression of the disease, stopping that progression and so-forth. So sure, the Korea rates don't prove Korea has magic dust that cures the problem but shows the Korean model is effective.
> If you're like the US and test very few you get the huge fatality rates we saw in Washington.
Most of the fatality rate in Washington is due to it spreading in a single nursing home. IIRC, it was 19 deaths from that one nursing home.
More vigorous testing comparable to SK likely wouldn't have caught the issue in this one nursing home in time as it spread like wildfire there. Only if the testing had caught the single employee that was the source would it have made a difference.
If testing were a huge factor, we'd expect to see a disaster in Japan, which is doing _very_ little testing. Instead, it seems to be doing even better than South Korea.
I think the masks are more likely to be having an impact.
i don't understand how knowing that you have the virus makes it less likely that you will die from it. There's no cure right? and at this point, anyone with a flu or cold will assume they have it and act accordingly, right?
It makes you less likely to give it to other people. Which makes people less likely to go to the hospital. Which makes the hospital less likely to run out of beds and equipment. Which makes the people with serious cases less likely to die. Which might even be... you in a few more days if you have a case that develops complications!
It also changes how people react and what they do.
Right now I see so many people carrying on their life as usual, because they think there aren't many infected people around them. That impression is a consequence of the lack of testing. It's likely that there are quite a few people around them who are sick and spreading this disease, and if more people realized that they'd act differently.
Resources and isolation measures are also directed to places where there are a lot of known infections, but if those infections are undetected very little gets done about them.
The relative lack of testing is a nightmare in the making.
You are correct, though though actually more complex than this.
1. Death from complications takes some time. You won't really know the real numbers until enough time has passed for the serious cases to resolve one way or the other.
2. Treatment makes a difference. Odds of death increase dramatically when treatment is not available.
No it doesn't. But what you ultimately want to know is the real number of infections. Testing is the best way to estimate that number. If you test just a few people you might e.g. miss a large portion that is either asymptomatic or is categorized as having a flu or cold. In this latter case, of course, the calculated lethality is higher than in the former - i.e. if you test lots and lots of people.
> If you could quickly and accurately test everyone in the country today we would know how to isolate and the whole thing would be over very soon.
i don't understand. let's say that tests are super accurate, a negative test result does not mean you won't spread virus in the future. You may have virus the next day or an hour later. tests are important for treatments but i don't think they are effective as a basis for isolation.
There's sooooo many lies being propagated by different governments on the true state of things. This afternoon I watched a live broadcast of parliament in which the minister of health claimed Belgium was doing far more extensive testing than any other country on earth. This at a time when standing instructions to medical personnel are to only test people that are already admitted to hospital because of severe pulmonary conditions. It is impossible to get a test under any other circumstance as all test request have to follow a central approvement procedure and non are approved barring these conditions.
These outright lies are propagated by the political parties that are far more concerned with 'the economy' than with any public health. It is really saddening that his is going on.
The surgeon general just gave a press conference in Baton Rouge with the governor of Louisiana saying we should only test people (or prioritize testing of) people with symptoms. This when we know asymptomatic people can be contagious for days.
The Port of New Orleans is testing embarking cruise ship passengers but not disembarking (!) ones. This when we have community spread in the parish already and have gone from 1 to 6 to 11 cases this week alone.
Your link is giving a 404. (It looks like it's pasted in twice.) And with regard to the cruise ships, see Question 13 of your linked FAQ.
It seems false positives are a real thing [1] but can we afford even one asymptomatic infected individual that might be a super spreader? In shifting away from containment are we just accepting these?
> People are thought to be most contagious when they are most symptomatic (the sickest).
Some spread might be possible before people show symptoms; there have been reports of this occurring with this new coronavirus, but this is not thought to be the main way the virus spreads.
Over here, the parliamentary debate was streamed publicly.
The instructions issued to medical personnel are also posted public.
There were HUGE discrepancies between those 2 sources of 'information', the quotes being added for the former case.
As such I have 100% certainty. I was validated later that night when despite our health minister claiming that 'we have it 100% under control' and our prime minister stating we were NOT going to be moving beyond 'stage 2' for now, a few hours later we moved to 'stage 3' and declared a national emergency.
Now for the speculation: Among those closer and more knowledgeable than me the rumor has it the health sector threatened the government to go public with the real state of affairs in the hospitals and in first line care if they would continue to refuse to take serious action.
As a UK citizen I am honestly terrified by my governments response and actions. In years to come I fear it’s going to be the textbook example of exactly how not to manage these types of situations.
I thought that - but then I watched today's press conference with the chief scientific adviser and chief medical adviser. They made some very good cases for not locking stuff down just yet.
Primarily you need to consider the behaviour of people. This is going to go on for a while no matter what we do and if we lockdown people now, by the time we hit the peak they will be ready to give up and go outside again. We need to save the drastic measures for the peak in order to spread the damage out and make sure they are effective. I was previously critical of the government but honestly I think it makes a lot of sense.
We need to consider the effectiveness of measures. Banning all flights into the US from Europe may sound like a grand plan but in reality it's not going to make a big dent and the economic damage is going to be huge. But it sounds good and in the current climate where we're being led by panic that's the plan people will like.
>> The resulting economic impact therefore can’t be that big.
The impact on the spread of the virus can't be that big either. My point though is that big flashy moves like banning all flights appear to do very little compared to more mundane tactics. At least based on the info in the press conference I'm referring to the data doesn't support flight bans, banning large gatherings etc.
You shouldn't discount the psychological factor of these things. Today, 1 day after the big move by the US to ban flights from Europe, we're seeing a lot more movement from various governments and states in taking action against the virus' spread. So even though the action itself might not be that useful, it's big enough that it gets people attention and it seems to have moved people across governments into more action.
True but I'd still go back to the UK advice: the virus is going to spread (we aren't going to stop it) so we need to focus on spreading the peak out so we can deal with it. If we force people to make drastic changes too early (well before the peak) then when we actually need them to make those changes (just before the peak) they will be burnt out and won't do it nearly as effectively.
Until recently I would have said the same thing as you, but I'm increasingly convinced that the drastic changes (closing schools, social distancing etc) are exactly what we should be doing to spread the peak out.
The peak is coming either way. Continuing to allow people to mix with each other as normal will make it steeper and more intense.
> We need to save the drastic measures for the peak.
If you only act when you hit the peak, any measures will be moot. Countries need to act now to reduce that peak and flatten the curve.
But sure, why not letting thousands of Atletico supporters into Liverpool, while Madrid has 1k+ cases. Was it also a "drastic measure" to play a football match behind closed doors?
> "Our aim is to try and reduce the peak, broaden the peak, not suppress it completely," he said.
> "Also, because the vast majority of people get a mild illness, to build up some kind of herd immunity so more people are immune to this disease and we reduce the transmission.”
They’re not acting only when the peak hits. They’re staging the response.
More serious measures come in as the number of transmission go up. And that’s all about managing the resources of the NHS over a long period of time.
Introduce lockdown now, sure, you delay the peak. But you don’t spread it out over a longer time period. People will stop caring and start ignoring advice.
I'd suggest watching the government press conference today where the chief science advisor + medical officer explain it. They explain exactly why you're wrong (and I'm more inclined to believe them after hearing them make the case).
Italy got caught by surprise - they only found out that they had cases when a 38 year old (!) walked into an ER with advanced symptoms. Given that this age bracket is not commonly affected by these harsher symptoms it is clear that they had long ongoing community transmission which has now culminated in the current catastrophe.
Germany is doing a bit better in this respect, it took them 1000 cases to 'get' the first death, showing that they have caught it very very early, due to their decentralized testiing system. That said, NPI must be ramped up significantly...
The US is maybe the most troublesome target for this virus in the developed world. A healthcare system that works well for few rich cancer patients is the opposite of what you want for a disease like COVID19.
It could also be cultural. Statements from Italian doctors I've seen said that their patients usually don't go to the hospital unless they really need care. That could've been the same here, people trying to sit it out until they needed intense care. In Germany, even people with very mild symptoms got tested early which helped to track down infections more easily. That also explains the low mortality rate.
Germany is counting deaths differently. If you have heart issues and you die due to a heart attack you're not counted as a COVID death. In Italy you are as long as you test positive.
> If you have heart issues and you die due to a heart attack you're not counted as a COVID death
That doesn't seem to be the case - a man from Baden-Württemberg, who died earlier this month, was only tested positive AFTER he was already dead for a few days and counted towards the statistic.
EDIT: I do not mean to imply that Italy failed in any respect. Italy has one of the best HC systems in the world.
The only reason this testing aspect worked out well for Germany is a very localized testing system. This type of 'federalism' is now a big issue though, as the gov can't simply ban events - only the states and communes can.
> Interestingly, that's 20% lower than in 2000 (3.04)
Almost the exact trend in Canada. I hope this is just a quirk of the data, because we would be screwed for this in 2000, and being at least 20% more screwed means we're extra screwed.
In effect, it seems that in Canada have fewer overall hospital beds per capita than Italy has acute care beds.
We are completely unprepared, and in terms of time, not far behind Italy.
That is a big factor. And: available nursing staff. Beds aren't enough. You need the right people to operate a large number of patients at the same time.
From what I read, medical equipment seems to be the bigger issue in parts of Italy right now. You can only convert beds to ICU if you have the right equipment. Nursing staff is obviously necessary but that doesn't appear to be the most limiting factor at the moment.
That disagrees with all the information that has been coming out of Italy for the last three days.
Perhaps because hospitals there (and in general) are always running at 80-100% capacity, so it didn't take much for the extra COVID-19 cases to max them out.
Indeed most EU ICU services are already usually running at around 90% with the usual issues (including the Flu). And please also do consider that most of theses cases are within the Lombardy region and that most ICU patients are very difficult if not impossible to transfer safely to other regions. While the ICU beds are limited, the amount of ambulances equipped with ICU equipment is probably even smaller (and will also require an ICU nurse+doctor on board during the transfer).
For instance, in my home town (Kraków, Poland), hospitals cancelled planned procedures yesterday - not due to the amount of COVID-19 patients itself (Poland still has double-digit number of reported cases), but because the hospitals run out masks, gowns and gloves. Which means that once coronavirus patients start appearing, things will get really ugly real fast.
This outbreak is a litmus test for the competence of countries. It's already shone a bright light on the fragility of global supply lines, cheap travel and open borders. These are the aspects of life most likely to change after this is all over.
>These are the aspects of life most likely to change after this is all over.
People will forget about this in a year and go back to life like it's always been. Short term convenience trumps everything except short term negative consequences.
No. I remember 9/11, and this feels worse. The world won’t be the same for a decade. Are you too young to remember when you could just walk straight onto a plane without being searched? Those days never came back.
From now on, a serious pandemic will never be some weird future scenario ever again. It will be a politicized issue.
We are seeing a real pandemic - something that has been the stuff of Hollywood movies for most in our generation. Maybe it's comparable in some aspects to the only other WHO-official pandemic: HIV/AIDS.
But this has an order of magnitude more impact on the entire planet and societies as we know them.
The stock markets look like load test graphs I see in Grafana every day. Steady ramp up and then after 90 minutes boom its over back to 0.
America is still not the same. I'm not talking about airport security, although that's a minor, minor difference. I'm talking about the government, the society, the culture. The terrorists won on 9/11 and they've been winning every day since. America is not a free country, if it ever was. The surveillance state has been ramped up. The police state has been ramped up. Wars have been ramped up. We started a war with a completely unrelated country and killed millions. Life for most citizens is absolute shit, barely making it by.
9/11 was not just a battle. It started a war the terrorists have been winning ever since. That's probably why there haven't really been any major attacks since then. Why try to attack America when us idiot Americans are attacking each other and bringing down the empire ourselves? The terrorists are just watching with glee.
The American ideal was land of the free and brave, and the writing at the Statue of Liberty welcomed poor refugees. But now Stephen Miller sits in the White House and is whispering Nazi ideas into a senile infant's ear.
I remember 9/11, saw the second plane hit with my own eyes. Other than airports and flying being more inconvenient nothing fundamental really changed as I saw it. People still traveled, people still flew and so on. Now you just budget an extra hour before a flight.
Geopolitics has seen massive impact since then. For example, the rise of ISIS is a direct descendant of the Iraq war which is a direct consequence of corrupt and criminal decision making by the Bush/Cheney admin in response to 9/11.
Debatable if the Arab Spring would have occurred without it, as the Middle East might have been much more stable.
Hear hear. And war refugees entering Europe is causing right-wing populism to rise (not that years of stupid austerity polcies was helping).
Would Brexit have happened without 9/11?
There's an ancient TIME article I have in my archives highlighting how the Dubya admin ignored Clinton's intelligence team's attempts to hand over info about the threat of a terrorist attack in the US. Would 9/11 have been prevented if Gore had won 2000? God damn hanging chads and rigged elections...
The TSA has been proven many times over to be totally ineffectual security theater - theres this popular report from a few years back that the TSA has a 95% failure rate when their measures are tested[1].
It doesn't go anywhere because there is now a lot of private industry in it for contract money to supply the spectacle whom have the lobbying power to keep it in place, but it is a total waste of money and gross violation of privacy for no positive benefit to society.
It's not the same stuff! Terrorism is backed by people actively wanting to harm other human beings, while the appearance of a new dangerous virus is a random process.
People stocked up supplies all over Europe when Chernobyl happened. This is not what we remember most. What we remember is "nuclear is dangerous". Some countries decommissioned their own power plants and didn't build new ones anymore. Example: Italy.
I'm sure that if everything ends well I'll remember being at home for a few weeks. I'm sure this is going to be a major turning point in history (more than Chernobyl and 9/11) but I'm not betting on what's going to be the direction it takes.
Re cheap travel and open borders, Jiangsu province, China is 300 miles from Wuhan, has 21 active cases, 610 recoveries and 0 deaths and presumably cheap travel and not much borders to Wuhan. On the other hand the US say is expensive to travel to and has a leader that goes on about closing borders, 2000 cases, 41 deaths and rising rapidly. The difference is competent policy not borders and cheap travel.
I'd like to hope, wishful thinking here, that there might be a trend towards requiring more scientific competence in our leaders going forward.
> It's already shone a bright light on the fragility of global supply lines, cheap travel and open borders.
Are you serious? Those are the things that have given us so much prosperity in the last decades, and indeed no government has dared interrupt the flow until it has become unavoidable due to majornational heath danger.
IMHO one consequence will be death of neoliberalism (started with Reagan/Thatcher but going philosophically to Hayek and Friedman). It is quite likely that U.S. will nationalize health care as a response to this crisis. But more broadly, the idea that government is a useless economic actor and shouldn't dictate economic policy will become laughable in the response to the crisis.
> It is quite likely that U.S. will nationalize health care as a response to this crisis.
If you think half the country infected with a virus and a million deaths is enough to topple a several hundred billion dollar insurance racket that has endured for over half a century exploiting health and wellbeing for profit...
I wish we would get single payer out of this, but the plague of greed in medicine is way too deep to be excised in a few months from a regular old viral plague.
I agree although the racket is more like a trillion. It is not just the insurance (payors) but also all the brokers and other rent seekers. I think there is 0% chance of nationalized health care in the US. Look at Obamacare; it didn't really work and took forever to get passed and most of the regulations have been rolled back. There are other things that I think could fix our health care and actually get passed and stick but Medicare For All isn't it. Too many in the US associate socialism with communism and think it unfair.
That mindset is a bit self-defeating, isn't it? I wonder if people thought we would have public schooling in the country 150 years ago, or that blacks could go to school with whites 100 years ago. Or that Germany would be the largest economy in Europe as a democratic republic, 70 years ago.
You are referring to the West African Ebola epidemic that started in 2014. There is also an ongoing outbreak in the DRC that started in 2018. That probably isn't receiving much international support right now.
I am not American, and there were infected people in my country. We had a right wing government then also, and since all the media is left wing here, they made an incredibly huge deal out of it. And now nobody remembers a thing.
It's been making the argument that Korea's aggressive testing has allowed them greater control over the epidemic.
Of course, there are a variety of other factors at work. Italy is the second "oldest" country in the world after Japan so Coronavirus infections just would be more deadly there. Also a lot of the Korean infections were confined to a single city in Korea (though the Italian infections also had an epicenter).
If Italy is the second oldest country in the world after Japan, how do they have 800 deaths compared to 16 in Japan? Something about those numbers seems off. Is it because Japan's elderly population tend to live in rural areas compared to Italy's or something else societally related?
meh. I've been married to a Japanese for over 2 decades now, and lived in Tokyo for many years including when Fukushima happened. I wouldn't trust Japanese politicians with their reported numbers any more as I'd trust China or the US.
There is one difference in Japan to Italy that might explain the lower infection rates: it's socially accepted to wear face masks (not only since covid but since the 90ies actually!)
Even if the numbers aren't reliable, reports of Japanese intensive care units being overrun aren't easy to hide, but Japanese hospitals don't seem to be under the same pressure as hospitals in Italy.
Making mask wearing more acceptable might be a cultural adjustment humanity has to make as we become more urbanized and globalized if it'll help reduce the severity of disease transmission. Looks like Japan's stumbled onto a very useful societal adaptation.
Japan's problem is a bit different -- it's estimated that there are 30+K old folks dying unnoticed in solitude every year (Kodokushi) in Japan, even without the Wuhan virus. As cynical as it may sound, that may be why Japan doesn't even bother testing their citizens for the virus.
FWIW. My wife is Japanese and I lived in Japan through Fukushima as well.
A lot of people seem to think that Japan must somehow have a higher infection rate but I haven't seen any evidence that this is true.
For all the docileness of the mainstream media and the lame-duck politics it is a free and democratic society. The government couldn't hide a mass outbreak of corona virus anymore than it has been able to hide any other scandal. In fact almost certainly less given the levels of public interest.
The Ministry of Health and Welfare publishes updated statistics daily (https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000164708_... -- in Japanese). looking at the current stats published there's not really any obvious problems. They're seeing about an 8% positive rate on corona virus tests and 1.8% of those with confirmed infections have died. This is well below the rates seen in Iran, Italy, America and China suggesting they've been relatively thorough in catching infections, although less so than South Korea.
In truth the Japanese healthcare system is probably the best in the world at providing population level care. Since long before Corona virus standards of hygiene have been very high. Masks and hand sanitizer bottles have been a common site for a long time, hand washing and gargling is heavily encouraged, and direct contact (hand shakes, hugs, back pats .etc.) is very restrained.
Whats more for all the criticism it copped the Japanese government has been pretty decisive in responding to corona virus. It's shut down schools. It's shut down public spaces (museums, libraries .etc.). It's discouraged crowds. It's encourage working from home. It's restricted travel from hot spots. It's isolated those with infections. Also most age homes seem to have gone into lock down weeks ago.
Japan for whatever reason has a pretty low testing rate. It's impossible to know if that is a confounding factor or not at this point. Their infection count/death count and test count are remarkably similar to the USA.
I'd speculate that Japan isn't in the situation of the infection getting out of control.
But none of posts should be construed as "Joe's complete model of Coronavirus dynamics." There are many things we don't know and can't predict. My main argument is every country needs much testing and much surveillance of the situation - IE, the Korean model is good, that is all.
Korea had people actively (hard to believe, I know) making things much worse. But they didn't downplay it for the first two weeks after the virus took hold. With these exponential issues time is everything.
"Of the 152 cases [article dated Feb 21] that have been found in the city, the majority have been linked to a [church], where Patient 31, a woman said to be in her 60s, is known to have attended at least four services before being diagnosed."
https://www.independent.co.uk/news/world/asia/coronavirus-so...
As of last night the number of cult-linked cases was "more than half". So > 3500. It turns out that in addition to worship services teice per week a lot of the cult members save money by living together. So even though worship has been stopped for nearly a month, new cult cases are still being reported.
I'm curious if something like this can be considered criminal. What if the mortality rate was higher? If the mortality rate was 100%, ethically would this be murder?
From what I've heard, the Sincheonji church had a long tradition of sending followers to other churches, hiding their identity, so that they make a lot of friends there, start small clubs and bible studies, and eventually convert them into their own church. (I even heard there were cases when they converted a pastor, winning over a church wholesale, though that might be a bit embellished.)
The problem was so bad that, even before the current epidemic, other "regular" churches had a sign saying "No member of Sincheonji is allowed in our church." So, yeah, not exactly your garden variety Christian church.
When you think about it, this behavior would make Sincheonji a perfect vector for spreading the virus. And that's what happened. Yikes.
They have over 200+K members now, but they are secretive in that they don't identify themselves as such when they recruit other church members.
Or worse, even after the outbreak, some didn't reveal their affiliation with the cult. In one instance, a dude leading Daegu city's outbreak management team, didn't reveal his affiliation with the cult until after test came positive and coworker were also infected. They also refused to give names of their cult members, even as most of new Wuhan virus cases were linked to the cult and the gov't actively sought their members for quarantine.
The buffet brunch was especially egregious because she came from the doctor's. She chose the buffet instead of getting a coronavirus test as the doctor suggested. And then she went on to a sermon.
age is correlated, not causal. there are simply too many other factors.
a generally compliant national attitude, combined with aggressive testing, and community-orientation probably had as much to do with south korea's success so far.
> This includes enforcing a law that grants the government wide authority to access data: CCTV footage, GPS tracking data from phones and cars, credit card transactions, immigration entry information, and other personal details of people confirmed to have an infectious disease. The authorities can then make some of this public, so anyone who may have been exposed can get themselves - or their friends and family members - tested.
I wish we developed this kind of capability so that we could opt-in. Wouldn't it be a hell of a lot better than nothing if 50% of the population chose to download the app, allow it to access our location and allow us to input symptoms and status, receive recommendations, then when this is all over, delete it?
I have visited several times and even before this virus I saw people wearing masks all the time. At grocery stores I remember seeing the workers who were stocking things wearing masks and gloves, which I never see in the US. Wearing masks while sick was already expected and has been for decades. Maybe since it's already in their culture to do what they can to stop spreading diseases, they were much better prepared than the rest of the world. They could also be lying, but that seems unlikely since the information would get out very quickly.
My hypothesis is that Japan, Hong Kong, South Korea, Singapore had to contend with earlier SARS outbreak and responded more quickly and comprehensively with contact tracing, social distancing.
I'm in Japan right now. I don't have any insight into government response, but there could be cultural factors that could have reduced the spread of the virus. In general, the Japanese avoid physical contact. They bow when they greet each other, money is exchanged on a tray rather than by hand, they typically don't hug, etc. Plus many people wear face masks. Occasionally when I bought something from a store, they would throw in a free face mask for me as well. And many businesses and restaurants put hand sanitizer at their enterance.
City or village, you'll need one where store clerks don't come in to work when sick due to lack of sick days and no one avoids testing and doctors for lack of insurance.
Italy's health care system has been overwhelmed - there aren't enough ventilators available for the people who need ventilators to survive and there are now a lot of them.
Italy's aging population has increased the proportion of people needing ventilators and the infection rate increases the total number.
Moreover, Italy's total actual infection is likely higher than the figures due to Italy's failure to test and control the situation. So the true fatality ratio is probably lower but hardly gives much comfort.
Japan simply isn't testing enough patients, so I would wait a few weeks before judging how well they did.
That said, inconceivably they don't have many serious cases. (If the virus was really spreading exponentially, we'd certainly see a lot more patients, tests or no tests.) So they must be doing something right. It's just hard to tell if they could keep it this way.
Italy is not admitting anyone over 65 or with comorbitidities to the ICU due to lack of space. That's not something you can hide in any open society. Nor is senior politicians dying like happened in Iran.
For whatever reason Italy and Iran are doing much much worse than any other country. My WAG is the wide spread use of masks in Asia is the biggest differentiating factor.
If you look at the ratio of test/positive people, and assuming that lower the ratio more wide spread testing is, Japan isn't doing bad. I don't remember exact numbers but when I looked at the numbers recently it was something like 3.5% for South Korea, 17% for Italy and 5% for Japan.
And note, I mean hit hard with high severity cases. Not just cases. My hypothesis is that it is already everywhere. Most of this exponential growth is just how fast we can deploy testing.
From my searches, they are currently at zero deaths? Low, at any rate.
Feels like this supports my hypothesis. If anyone starts looking, they will find cases. Only if you have a baseline lung damage rate that is elevated will you see severe cases.
Yeah I'm curious myself. It seems like no specific policy can clearly explain the results. IIRC Japan is one of the later countries to restrict travel from China back when cases were high there and in general did limited testing on their population.
Maybe the public hygiene practice and culture of wearing masks really helped, or maybe the infection is still developing there.
My guess is large city: possibly better health services, possibly higher priority if supply lines are affected. I don't think population is a big factor as long as you isolate yourself, since even in a small village, if someone is infected, it'll eventually get to you if you're exposed. Not an educated guess though.
A small village/town; away from the urban craziness; where you can walk over to your neighbor’s to ask for a pound of dried beans because the just-in-time retail model and cascading supply-chain effects means your local grocery store shelves have been emptied of the staples.
> A small village/town; away from the urban craziness;
Considering the fact that we both were downvoted, that's not the answer they want to hear on this forum. In a way, it was to be expected, since the majority usually praise density each time an urbanisation thread comes up and consider metropolitan concentration equals progress.
All the years I lived in cities and did what an average urban dweller does: packed in an office, packed in public transportation or even packed on the pavement, packed in shops, packed in bars, packed in elevators, packed on the terraces or in a concert hall; I was getting a flu (or something very similar putting me in bed for 3 days) at least twice a year, sometimes thrice.
In the last 7 years, I have been living in the country and not taking part in almost any social activity. I got my first major flu on January this year. First time in seven years for something that previously happened to me every year. Brought by family members who had gone to some gathering... in the city (and who had been vaccinated against flu as obedient citizens, but that vaccine is notoriously crappy). We all got sick. In all those years, I only got 2 or 3 minor episodes, and all of them immediately followed one my very rare and short stays in the city, or a close family member who brought me that 'gift' from the same place.
Same, but with the cold. The cold affects me severely, I remember the last time I had the flu over a decade ago, I really don't want to experience that again heh.
Living in a big city you're just exposed to more people, you're just more likely to catch something
>Epidemiologists say it is not possible to compare the numbers directly. But some say the dramatically different outcomes point to an important insight:
Don't compare these numbers....but if we do it anyway...
S. Korea is very interconnected as a society. Technology does have a role but people are generally receptive of personal information being collected and used. For example, in order to hand out the proper number of masks, they have APIs which allows a database to inventory pharmacy mask handouts. In the face of a crisis, are Koreans forfeiting their privacy or are they trying to curb a bad situation? Americans would definitely not tolerate any info sharing and now there are strict laws against information collection.
Yes. They're generally quite compliant and community-oriented as well.
If the health minister says the best way to slow this is to stay inside, then generally they'll stay inside.
Meanwhile, I have friends who are giving the middle finger to caution and are heading off on their flights for spring break - all for the privilege of being carriers.
I'm curious about the cultural differences. Physical contact, kiss on the cheek, is much more common in Italy than in Korea. That can play a huge factor.
Koreans rarely hold hands in friendship too. Shaking hands, etc. You bow instead. When you go on a date, you're lucky if you get to hold hands on the first date. Kissing in public? Unacceptable.
Well, yeah, but go to a restaurant in Korea and everybody thrusts their spoons and chopsticks into shared side dishes and soup bowls. That must count for something. :/
S.Korea is also effectively an island - water 3 sides + sealed N.Korea border. I don't think it's useful comparing large interconnected EU countries response capabilities against Asian Tigers islands (Korea, Singapore, Taiwan) with deep collectivist cultural roots and large demographics that still remember living under centralized authoritarian rule. In the case of Singapore and China, still are.
Italy has too much travel, old demographics and interconnected borders to respond the way Korea did. And we don't even know if Korea is out of the woods yet, they got more clusters recently.
> [...] deep collectivist cultural roots and large demographics that still remember living under centralized authoritarian rule. In the case of Singapore and China, still are.
From Singapore's Wikipedia page:
> Freedom House ranks Singapore as "partly free" in its Freedom in the World report,[137] and The Economist Intelligence Unit ranks Singapore as a "flawed democracy", the second best rank of four, in its "Democracy Index" [1]
Singapore is a flawed democracy, just like Hong Kong. Its unfair to mention it in the same breath as China which, according to the mentioned index, is Authoritarian.
It's a valid comparison in the sense that both Singapore and Chinese governance structure allows extremely despotic interventions that other representative forms of governments cannot. The broad point that the countries that responded effectively so far either have the benefit of authoritarian mobilization capabilities or still have vast populations that experienced living under the shadow of authoritarian regimes. I don't think we'll see similar levels of compliance in the west, on top of actually having very difficult borders to police.
Your last line is the super important point, occurred to me today as well. If we beat this thing with social distancing, idiots will say "See! There was no reason to panic!"
Indeed. Just 2 days ago I was talking to someone who was annoyed by people taking measures: "See, in China they're already seeing infections going down! No point in taking all these measures!" Without apparently realizing the reason why they're going down is extreme is precisely those extreme measures.
The problem with local, less aggressive measures is that people act in their self interest to bypass them for convenience or safety, and they make the problem worse. Recent examples:
- Lockdown in northern Italy: People ran to the south taking the virus with them.
- Schools closing, folks asked to work from home in Madrid: Families drive to the coast where bars and restaurants are full.
I agree that in a place where compliance with social distance measures is high (I'm thinking South Korea, Japan), that would be enough. But that doesn't work everywhere.
The big issue we have seen with contact tracing in this pandemic is that it doesn't catch everyone. Those contacts you didn't find start new chains that you need to find and disrupt, but doing that requires more tests than are available: People who haven't been traveling are simply denied tests. So you never find those chains, and you get out of control community spread.
I think it is fine to let the idiots win on this one and rub it in our face forever. I would be willing to boost the ego of anyone if we can contain this.
I mean if we have arrived at a point where majority of the people can't be convinced of the existence of this, and the only way to make them understand is to do some damage, we have bigger problems as a society in front of us. You don't throw a kid under a bus if he doesn't understand you, you just keep trying with incentives and maybe minor punishments.
You do understand that everything would have been fine if we simply pretended this virus didn’t exist, right? A few extremely old people would have died slightly sooner. That’s it.
No, that is totally wrong. The medical system would collapse. See what is happening in Italy. Most of the critical cases require ICU. There aren't enough ventilators if everyone gets infected. And without proper care, not just old but even young people may face huge problems.
The disease is extremely contagious. Hospitals would've been even more overburdened as they currently are if we just "did nothing" because it would've spread much quicker.
You might get to the point where you need to make a choice between who you're going to accept in the hospital (younger people then get the fast lane over the elder due to potential higher amount of life years being saved). I believe its like that in Italy at this point.
If old people quarantine themselves the chances of them not getting this disease increase. I know a few elder (including loved ones) who I don't want to see passing away, so I have an interest in this.
On a different note, I also find it selfish and distasteful to feel careless about big groups of other people based on discriminatory elements such as age.
Whether it's social distancing or some other factor, the important point here I think is that it wouldn't have died down on its own. For you to look at the positive outcome alone and say "see, it wasn't a problem to begin with!" is just as irrefutable as to say it was the social distancing. So you have to use understanding of the disease, logic, data from other countries, etc, to come to your conclusion.
(You ask an annoying, but fair and important question here. We shouldn't lose our skeptical mind.)
The claim is not that if it dies down after social distancing, therefore social distancing was to blame, but that if it were to _really_ die down due to it, the measures would seem like an over-reaction to a certain segment of the populace. I think that, while a bit presumptuous, will hold true.
But, these measures need to hold on for long enough, until all reservoirs are depleted. Relaxing the measures after the transmission rates decrease will only stop it temporarily, so it will flare right back up if it has a source that was missed.
Also, the lower the R factor, the faster measures can be relaxed. With an R0, if you want to guarantee putting out everything, you need to hold the measures for the longest possible lifetime of the disease. ( what's that? A month?)
I’m wondering what fraction of little kids already have it and are serving as essentially asymptotic vectors. Once a large enough fraction of little kids are immune or resistant, r0 may be permanently reduced.
That's my thought as well. With having a vaccine like 12-18 months away at best, is there another strategy than just trying to eradicate it in a _massive_ concentrated worldwide effort?
I think all the current measures are for the purpose of curve flattening. The volume under the curve (infected people) will be the same but it will be spread over a longer time period and hopefully avoid a spike of cases that will crush health care systems.
Unfortunately that math doesn't work. The US has roughly 100k ICU beds. Critical patients are spending about two weeks on a ventilator. Doing the math that means we can treat a maximum of 2 million patients this year.
Assuming half the country gets infected and the 20-30% hospitalization rate remains that's 35 million or so patients.
So best case we can treat about 5% of the cases. And that's if we let no other patients into the ICU. Which isnt practical because they run at ~80% capacity or more anyways. So really that number drops down to more like 1%.
The only option is to contain it or watch millions die.
Does anybody have opinions on outdoor activities in small groups? Supposing we've come to the point where we're otherwise staying at home where possible. It could get psychologically daunting, especially for those of us who live alone. (Video conferencing could help as well). I thought some outdoor games with people in real life, maybe 10-15 people, staying a meter away from each other, etc. Is that small risk, miniscule risk, significant risk?
At my jiu jitsu club, we're moving into no-contact grappling. This will keep us safe from the virus yet give those in quarantine some much-needed mental relief. See e.g. https://streamable.com/loz3v . Don't do that outdoors though, unless you can find ways to avoid the injuries from no-contact grappling on hard surfaces.
What's interesting is, many South Koreans still believe the South Korean government is to blame. Perhaps no people are satisifed by their government?
Usual counterarguments are like these:
1. The government should have prevented the entry of foreign nationals who recently visited China. It could buy us some time to develop treatment to the disease. To this day, no such ban has been imposed.
2. It should have prohibited masks from being exported in January. Many masks are suspected to be exported to China, which is believed to have contributed the scarceness of masks. Thankfully, the exportation is banned now.
3. The government shifts a little too much responsibility to the cult. In addition, some people blames Daegu, where the cult made thousands of people infected, for not handling the situation properly, to prevent the central government from being blamed.
But after seeing the reactions of other countries, I'm starting to believe South Korea's actions were actually pretty good, at least relatively. What do you think?
Counterargument #1, #2 is due to the government's stance towards China. The government is trying to win back China's (so called) friendship, which was shattered when the U.S. deployed THAAD there.
South Korea was able to handle this not because the government did good, but they experienced the MERS outbreak in 2015. Legislative measures to prevent outbreaks were made then. (plus the lesson of impeachment I guess)
Korea is doing some robotic testing of the samples:
> Rather than a human mixing the solutions, the samples are instead put into a diagnostic machine. Inside the machine, a robot arm pipettes the solution and mixes the liquids on a number of tests at once. According to Chun, this method takes only four hours to test samples from 94 patients -- four times faster than the manual method. It also reduces the risk of human error or contamination.
I think a lot of places are probably using automated testing machines. Apparently, Public Health England has been operating theirs 24/7 after the staff go home to keep up with the incoming samples, and that's one reason why results take a lot more than 4 hours.
Its not tests we should be counting but the number of people seriously sick and work back from that.
If we know that a percentage of the population will get hospitalised we can get a good estimate of the actual infected population.
I think that the UK estimates that 10K people have it in the UK for example. (Number may be wrong, but they have produced an estimate based on the number of sick who tested positive)
The UK is basically saying, currently, to not expect to be tested, that you will get it and that they have good knowledge of the levels. They are testing sick people in hospitals only. They also say that advice is likely to change each week.
I do not know how south korea managed to get as many test kits as they did, but Italy (and the rest of europe, the us, everyone except south korea and singapore) simply do not have enough testkits to be able to copy them. So instead we have to limit the spread by telling people to work from home. Also Italy found out they were infected much later than south korea. people estimate the virus had been spreading for weeks when they did.
Anecdotally, my younger sister spent last year as a foreign exchange student in Modena (northern Italy). She explained that she's not surprised at all about the impressively quick spread there as nearly everyone she knew and interacted with greeted each other with two kisses on the cheek! I can't imagine how difficult it must be to contain a virus with such deep ingrained cultural norms.
US is pretty much headed for the italian model thanks to almost non-existent leadership and people unwilling to isolate themselves, feel the right to go everywhere public while sick and cough/sneeze on everyone
A month from now there are going to be so many people sick, hospitals overwhelmed and they won't be able to hide the death count anymore.
My understanding is that the epicenter in Korea was a church whose audience skews young, which has affected the mortality rate there. Basically, if you have a bunch of young people get it, your mortality rate will look lower than if it spread through an older segment of the population.
> They are testing hundreds of thousands of people for infections and tracking potential carriers like detectives, using cell phone and satellite technology.
No but thanks. I do not want to allow a spy-state that might stay after the virus is sunset.
It's not just the number of cases that differ due to different testing regimes. Another difference is that Italy did some post-mortem testing to identify cases that were wrongly reported as flu etc. but were covid19. I assume they were included in the number of dead. I don't know if they did the same in South Korea. Numbers sometimes are difficult to compare.
You can be infected without having a fever. That's one of the problems with coronavirus.
Knowing you have the virus won't save you, of course, but you will be able to react accordingly. That will include trying not to infect anyone else....
Is there any map of the spread within Italy (or any other country) region wise, so that one could see how effected different regions are, and how region wise quarantined have worked.
Is there a site that comments on general news, has an educated audience and debunks spurious or dubious claims? I’d like to read my news through such portal.
The reason HN works (well one reason) is vigorous moderation and a stamping out of any mode of discourse apart from collegial intellectual discussion. As a result, we don't see memes or most of the other cheap humour you will find on e.g Reddit. It also seems to lead inevitably to people whining about downvotes, and to people whining about people whining about downvotes.
HN is basically ideal for analytical, logic bound folks, and it works because the topics tends to be things that we can reason about and evaluate using logic.
HN would not work if the topics were more general. Anything political for example seems to hardly lend itself to logical discussion. It's impossible to imagine a @dang enforcing civilised discourse on political discussions.
How about Occam’s razor? A much easier explanation be we err on the number of infected people. Tests are one way to approximate the number of infections.
One tangential snippet that I heard but I don't know if it is true or not is that in Northern Italy, there are whole garment factories that are staffed and possibly owned by Chinese purely so that they can be designated as Italian clothing manufacturers.
You're absolutely right. It's been an ongoing part of day-to-day life for Koreans. Fortunately, things are pretty transparent and there aren't big businesses trying to monetize on this information (but this may change in a flash).
If that’s truly the case, privacy and freedom kind of need to step up their game. I feel like parts of asia are handling this much more responsibly than the US and Europe.
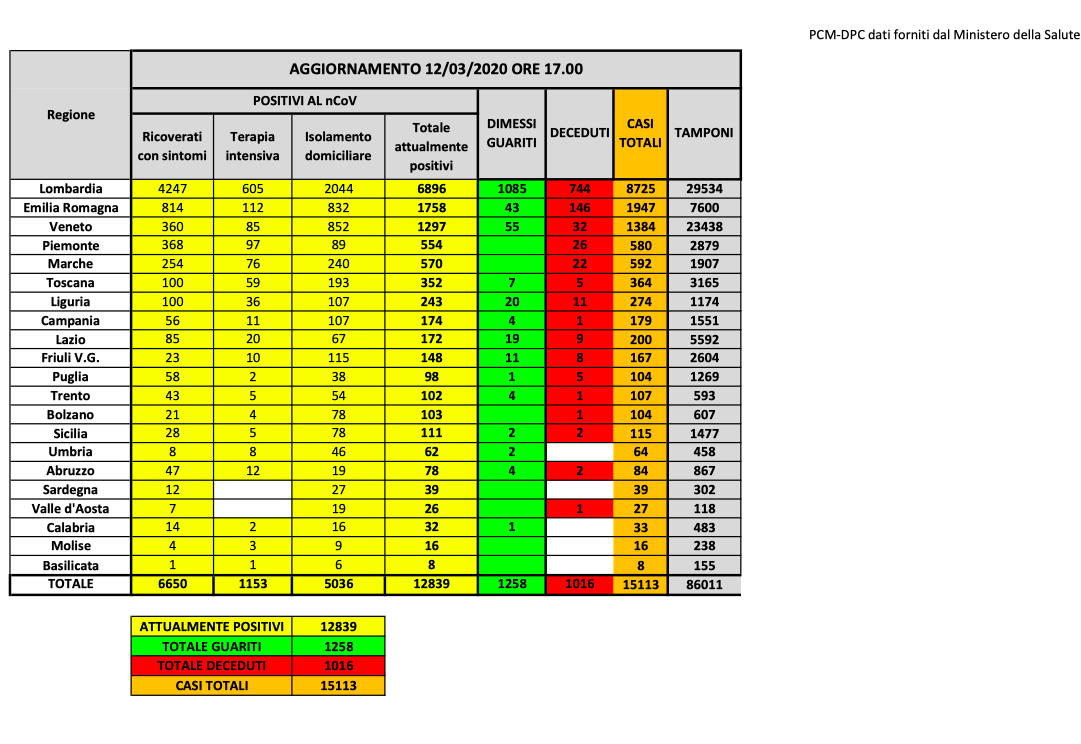{kind=link}
- Average age of death due to Coronavirus in Italy is 82 [1]
- In Italy, 3.65% of the population is 80 or older [2].
- In Korea, 1.75% of the population is 80 or older [3]
[1] https://www.epicentro.iss.it/coronavirus/bollettino/covid-19...
[2] https://www.populationpyramid.net/italy/2019/
[3] https://www.populationpyramid.net/republic-of-korea/2019/