7 people out of 7 million dose's. That's why they stopped. My wife and I got the J&J shot on Saturday so I'm directly at risk and I'd take it everytime even if the risk was 10 times what it currently is. I've already seen a bunch of anit-vaxers referring to this in new articles this morning. So let's see, 1 in a million chance that the vaccine will make you sick (only 1 person has died so far, which is terrible but it's 1 out of 7 million) vs a worldwide pandemic that has killed millions. All these anti-vaxers talking about living in fear of a virus that has 98% survival rate are AFRAID of a vaccine that has a 99.999998% ( 7/7,000,000 == 0.000001) survival rate, oh and is 100% effective at stopping you from dying. Literally no one that has received the vaccine has died from COVID19. The fact that modern society can be SO smart some times and yet so incredibly idiotic is so frustrating to me.
I think it is a disservice to outright label people as anti-vaxers simply for questioning the risk-calculus of vaccines. The (1/7 million) is the current, unconditional and empirically observed adverse effect of the vaccine - this is a somewhat noisy measure of the true prevalence of this issue. It is okay to be cautious and there are legitimate concerns, and quite frankly, I trust the FDA have good reason to pause this if Moderna/Pfizer are readily available anywy. In countries where there are not alternative vaccines available, the risk calculations change, and as such, you might be better off taking J&J or AZ. In any case, to your earlier point of why they stopped it: they didn't stop it because (7/7 million), they stopped it because it was not observed in the trials and now they have to recalculate the risks for various age-groups and inform people, accordingly. If these events were observed in the trials and the prevalence was the same (in trial, and out of trial) then it would not be a cause for concern.
> The (1/7 million) is the current, unconditional and empirically observed adverse effect of the vaccine - this is a somewhat noisy measure of the true prevalence of this issue. It is okay to be cautious and there are legitimate concerns, and quite frankly, I trust the FDA have good reason to pause this if Moderna/Pfizer are readily available anywy.
How many injections do you personally need to feel comfortable? Seven million people is way more than any clinical trial for any drug you've ever taken, and I guarantee you any of them is more likely to kill you.
Every single year 150 people die from taking Tylenol in the US in the normal course of treatment -- and 500 die of acute liver failure due to acetaminophen overdose. 25,000 hospital admissions. 50,000 ER visits. If we pretend that 350,000,000 people take Tylenol each year, that makes Tylenol 50% more likely to kill you than this vaccine.
This comment is a prime example of why we’re in this mess with vaccine denial in the first place. You’re either not allowed to say anything negative about vaccines, or you’re an anti-vaxxer who thinks your kids will get autism and 5G chips. It’s so cult-like.
We should be honest about the (low) risks and benefits of vaccination without turning it into a political campaign of shame and bullying, and trust people to make the right choice for them and the public.
Exactly this. A lot of conversation seems to ignore how humans behave. Pausing, examining data and restarting with updated guidelines further encourages confidence in the process.
Imagine if the FDA says "no big deal, low chance of it happening, keep going", then a week from now "oh seem like the rate has doubled, still low, keep going", then a week later "ok, if you have any risk of blood clots don't take the J&J vaccine". That scream "we didn't think this would happen".
You've just eroded trust in the system and the next time some weird side effects comes up you won't have to pause, people will just refuse to take it.
IMO, no - I'm saying that folks risk management is completely out of wack. The chance the disease kills you is 1 in 100. The chance that the vaccine kills you is 1 in 7 000 000. One is bigger than the other. By, like, a lot.
The government's response is to pacify anti-vaxxers.
I’m 25 and I’m relatively healthy. The risk that the disease kills me is significantly less than 1 in 100; it’s hard to find numbers but one chart had the hospitalization rate for me at 1%, and the death rate 0.01% (edit: though the death rate only covered age and didn’t divide by other factors such as obesity). The “chance” the vaccine kills you is currently zero as there have been no recorded deaths that have been linked to a COVID vaccine. The blood clotting risk has been cited as 1 in a million, but we’re working with limited data. This is the problem with making such extrapolations.
I write all of this as I’m on day 2 of dealing with the side effects of J&J.
The reason everyone has to get it is so that the average goes down to 0, for everyone.
7 million trials is not limited data. It's dramatically, and I do mean dramatically more data than basically any other clinical trial for any other drug you've ever heard of. By probably 2 orders of magnitude. It's simply not limited data.
The average phase 3 trial has 300-3000 participants [1]. Not seven million.
It's 6 in 1000 if you listen to the CDC; personally I think the real number is closer to 3 in 1000. That's not too far off from what you said but I prefer being more explicit rather than using such a fuzzy resolution.
And just to be explicit, that's the general IFR, the IFR for, say, people in their 20's, or even people in their 40's, is a fraction of that.
---
Anyway, your point about risk management is somewhat true, but it is much more true if you apply that logic to the general public's fear of SARS-2 in the first place. I can't find it in my notes but surveys that have asked people what their chance of dying is if they catch the virus, are off by MULTIPLE orders of magnitude. And young people rank their individual risk of death higher than old people do (both estimate too high, even the old people), presumably due to them being more "plugged in" to "the system" so to speak.
Personally speaking, since I'm in my 20's, almost everyone I know who has gotten the vaccine has done so because they believe outright falsehoods about the virus that have been propagated not just by the media but by our so-called health experts themselves.
For example, I have multiple friends who had PCR-confirmed COVID-19, recovered months ago, and still got the vaccine. In the times I've probed at them to see why, they muttered some vague things about "the variants" and essentially said that the variants bypass naturalistic immunity which is just completely false.
I know for a fact that my likelihood of an acute adverse reaction (the all-too-common "feeling like death for a day" reaction) is far higher than the likelihood of comparable symptoms from SARS-2 infection. So I'm not getting the vaccine, and I'm not embarrassed to say so. For many people, the risks of the virus are less than risks of the vaccine; however, much less people than you would think. We don't have good enough data yet but I'd bet it crosses over somewhere in the 40's or 50's age range.
There's a huge difference between being an "anti-vaxxer" in the true sense of the word - i.e. you think all vaccines are inherently bad, period - and being someone who takes the same attitude towards vaccines that we do towards drugs: no drug is inherently safe; rather drugs that are proven to be safe are safe. By extension, no vaccine is inherently safe; vaccines that are proven to be safe are safe.
The latter statement is my personal view of it, and unfortunately such a statement can get you banned from social media platforms if you get unlucky.
This binary way of dividing the world into "anti-vaxxer" vs not, "AIDS denialist" vs not, etc is not just oversimplified but is intentionally done to suppress dissent. I refuse to participate in such a culture and I humbly implore you to do so as well.
> How many injections do you personally need to feel comfortable? Seven million people is way more than any clinical trial for any drug you've ever taken, and I guarantee you any of them is more likely to kill you.
Again, the point is, when we observe adverse effect in the out-of-trial phase, it has hard to pin-point cause and effect. It is not a guarantee that the 7 million necessarily represent a random sample so proceeding with caution is warranted. We know, for example, vaccines have been distributed by age, and chances are, the 7 million is bias towards the older demographic.
> Every single year 150 people die from taking Tylenol in the US in the normal course of treatment -- and 500 die of acute liver failure due to acetaminophen overdose. 25,000 hospital admissions. 50,000 ER visits. If we pretend that 350,000,000 people take Tylenol each year, that makes Tylenol 50% more likely to kill you than this vaccine.
Again, the point isn't that {insert_your_favourite_drug} is 10x more likely to kill you - the point is, when we do not understand why something is happening, it is better to pause and detect whether there is a more fundamental issue. For example, suppose that every single injection that caused an adverse reaction was produced at the same facility and as part of the same batch - we would definitely be better off in investigating the root cause than to leave it be. Until we fully understand what mechanism is causing this adverse effect and how to best counteract it, in my opinion, a pause is warranted.
Sure, in isolation, that's all true. However, in isolation, the cost of doing nothing is zero. In a pandemic where 70% of America will catch a disease somewhere between 0.3% and 1% fatal, the cost of doing nothing is dramatically higher than zero. In fact, it's dramatically higher than a vaccine that just randomly kills 1 in 1,000,000 people - which this one strictly does not.
My point is that yes, an investigation should be carried out, but stopping the trial obviously - trivially - does more harm than good due to the extenuating circumstances of the global pandemic.
Agreed, I've had all other vaccines, but this batch is rushed, experimental, and not necessary for me - labelling people such as myself "anti-vaxers" is just dishonest, bitter, childish, name calling. Very few people in my area of London have bothered with the so-called lockdown (too much was open to be called a lockdown), masks, etc - I expect I've had all variants, and apparently my immune system is on top of it, in which case there's nothing to pass on; and the people in my area clearly don't care if I did. I'm no more an "anti-vaxer" than I am an anti-martian.
Did you get an antibody test to confirm that you've already had it? I don't think data supports the assumption that you've already had it; it's a rare disease even where it's spreading widely. I also have a gut feeling that people didn't take "lockdown" or social distancing seriously, but some counterevidence is that nobody in the UK has gotten the flu in 2021: https://www.independent.co.uk/news/health/flu-cases-covid-en... That's not because they're already immune, it's because diseases simply aren't being transmitted. As bad as people are about masks and social distancing, there is some measurable effect.
I'll also point out some anecdata. I know someone in their late 20s that got COVID. They have felt miserable every day in the 9 months since having it. Others have relayed similar stories. Public health authorities are worried about severe consequences like death, but death isn't the only possible outcome. You could just feel like shit for the rest of your life.
To me, this is a nasty disease that I do not want to contract. I probably won't die if I get it, but there is more to life than merely not being dead. As a result, I got the vaccine as soon as I could.
Well, you may not be (or see yourself) an anti-vaxxer, and your right that it's not necessarily wise to label everyone as such who have concerns with these vaccines, but it also doesn't mean that your excuses make sense.
The batch is not "rushed" more than it's needed: there IS an emergency. It's also not experimental. The experiments have all been done (up to phase 3). It's perfectly normal to only see 1 in a million (or even 1:100 000) side effects after starting the vaccination of the general public. Simply because the phase 3 will never contain millions of people. I've checked, and the 30-40k studies we had with these seem to be indeed large. I.e. safe.
What you think about your immune system is kind of irrelevant for a few reasons, but talking up their immune system seems to be a general self-convincing strategy for a lot of people. First of all, it's not apparent that you have contracted the virus. Unless you have an antibody test showing that you are seropositive, you simply don't know, but the chances aren't very high. What you can be sure about is that you have not contracted "all" variants. If you live in the UK then you had the chance to meet the UK variant (B117, IIRC) and the base variant (D6.... whatever). Very likely not both. And the immunity for the base variant seems to work pretty well for the UK variant, so it doesn't even matter if you met both.
But even if you know you are already immune, the natural immunity doesn't last that long. The vaccines give you higher antibody levels (at least the mRNA ones do, again IIRC) and better immunity especially due to the second dose. (Which you can't really simulate with a second infection within a few weeks.)
And at last: you can't generalize from your own experience. Looking at the numbers, which we do have a lot of, people who haven't met the virus and don't have immunity should by all means get the vaccine. Because the virus is a lot more dangerous (several orders of magnitude more dangerous) than even the J&J or the AZ vaccine. Though the exact risk profile will depend on individual factors, of course, but since you've talked about all vaccines...
Zero experiments have been done on long-term effects, and you cannot, and no one can, counter this point.
That's the definition of "rushed".
Vaccines typically take several years of testing before being approved. These aren't approved according to those standards. Manufacturers are absolved from risks because of this "emergency use" status. Why absolve them if there are no risks? If they truly believed these were safe and of tremendously important benefit, they could stand up and say "we accept responsibility for negative outcomes in accordance with ordinarily approved medication, and waive our rights to emergency use protections". Then everyone would rush to take them as doubts would be broadly eliminated.
Things are "rushed" because it's an emergency. SARS-CoV-2 has existed for a little more than a year, and it's already killed 3 million people. At some point, you have to take the leap of faith that this thing that's very much like other things is going to actually be very much like those other things. mRNA vaccines are not new. Adenovirus vaccines are not new. Vaccines are brought to market in less than a year routinely; consider the seasonal flu vaccine.
(Why are we seeing mRNA vaccines for COVID and not other diseases, if it's not new technology? Because the vaccines for other diseases didn't work.)
You are totally right that there could be some magical protein in the vaccines that causes you to drop dead in two years. There probably isn't though, so what you call "rushed" other people call "saving lives".
9 million - including many children, and mostly people of colour - die each year of starvation. Where's the emergency, trillions and unprecedented worldwide cooperation and effort to eradicate that forever within less than a year? It doesn't even require the invention of anything new, and is primarily a logistical (/expense) problem. Would save three times as many lives just in the first year, overwhemingly more life years overall, and be much easier to implement, being confined to mainly a few known, poorly-resourced areas (rather than the entire earth).
If you've seen or lived the effects of starvation firsthand, you'd find it difficult to understand why suddenly everyone is willing to do anything, even destroy their own livelihoods or take rush-developed intravenous shots, to try and save the lives of a significantly smaller number of predominantly elderly people who were about to die of just about anything else anyway, at the expense of those 9 million (or any other of preventable causes of death that kill in higher numbers per year and have been known about for decades, for example: smoking).
Why not spend a year making the manufacturing of cigarettes illegal, have a worldwide crackdown with cigarette company executives hauled to jail for crimes against humanity, make it illegal to depict smoking in any media, censor all images of cigarettes, and launch a 24/7 every news channel, every street corner propaganda campaign, with celebrities publicly blacklisting smokers?
Save significantly more lives in the first year, and keep doing so year after year. Wouldn't need to trash the economy, ruin businesses, or risk plunging anyone into poverty, etc - and no need for anyone to take a rushed, long-term untested shot.
> 9 million - including many children, and mostly people of colour - die each year of starvation.
The sad thing about this kind of argument is that it never goes away. Whatever happens. I started an argument more than a year ago with a guy, when we had 3000 deaths. World wide, total. He kept saying that it's less than the number of people who die in car accidents in a day. And he was right. What he didn't get is that without counter-measures it would grow exponentially for quite a long time and to quite a large total.
And it did grow and we continued this argument for months (with 1-2 comments a month) he had to keep raising the stakes. Next it was less than the number of flu deaths per year, next it was less than the number of car accident deaths, this time per year, then the number of HIV deaths, and then he just stopped arguing. I pinged him at 1M last June, never responded. I don't think he changed his mind.
I see your argument as a continuation of that. You just raised the stakes again, but however much the total count will be, you guys will always find something bigger. Implicitly stating that it's only worth taking counter measures against the worst cause of death. (Be it lockdowns or vaccines.) But it doesn't make sense. This is ON TOP of all those. Also, let's not forget that the only way we managed to keep it down to 3M is by imposing pretty strict lockdowns worldwide. Without those it would have been a lot worse. And even with these lockdowns the health care system is waaay overloaded in a lot of places, which means that COVID kills indirectly as well.
Yes, help people who are starving: we can easily do so by donating money. As long as you have the money. But don't make it worse by not vaccinating and letting COVID kill others, kill even those who are very poor (they definitely have worse chances) and kill the economy which obviously means more people starving and less help for those who have already been starving.
9 million/year have not been helped by donations, that's why the number persists.
The "per year" number for COVID cannot change now, it's been a year. It is what it is.
COVID, in light of other preventable deaths, and especially in terms of life years lost, is not of justifiable greater concern compared to others, and from mortality rates/demographics and seroprevalence, this has been broadly known from not long after the beginning. The dollar cost versus life-years-saved is borderline insanity.
The argument lockdowns saved lives has been thoroughly debunked [0], and even the most cursory common-sense look at any per-capita chart by country and measures employed confirms that at a glance.
If you want to continue killing tens of millions per year so you can save the lives of far fewer, you have no standing. Frankly, that position disgusts me.
> 9 million/year have not been helped by donations, that's why the number persists.
I don't know where you are getting with this. As I said, this is at best an independent problem that can (and should) be handled. In reality it's worsened by the pandemic.
> The "per year" number for COVID cannot change now, it's been a year. It is what it is.
Though I think I didn't say the "per year" number would grow now, you are actually wrong for two reasons:
- while it's been a year, the beginning of that year was pretty mild, less deaths per day than during the summer or these days. So as we move the window, actually the per year number will increase. E.g. if you look at the "total deaths" graph on Worldometer [0], you'll see that it ramped up around the middle of October. It accelerated about 2x (but at least 1.5x).
- we got these "wonderful" results with various restrictions. And you are agruing for no restrictions, but you can't prove that no restrictions wouldn't yield much worse numbers.
> in terms of life years lost, is not of justifiable greater concern compared to others
I've already responded to this: it doesn't have to be a greater concern. It's a preventable concern. As far as I can remember, we were talking about vaccinations.
Also, years of life lost changes as the epidemic goes on and as the virus mutates and seem to get more aggressive (which is an affect of breeding it in a large number of humans). And let's not forget again, that the numbers are affected by how much the health care system is overloaded. Young people will die if they can't get into a hospital because too many people get sick at once.
> The argument lockdowns saved lives has been thoroughly debunked [0],
Yeah, I know. The whole pandemic has been "debunked" quite a few times. The first "debunk" I've read was a year ago, when a guy started lamenting that it would just die because of the network effect. It didn't. I've checked one random article from your link. It looks pretty weak. It just says that no matter what, the epidemic wave just stops after 6 weeks, because that's what it does. It lumps together countries like Sweden and Taiwan, which is crazy in its own right, because Taiwan has 11 deaths/30M people today and Sweden had like 8k/7M back in June (IIRC that's when that article was written). Needless to say, with the 3rd wave in Europe, the 6 week rule is out of the window: our 2nd wave (here in Hungary) was in a decline in mid February, when it started to rise, probably due to the spread of the UK variant. Without any change in the lockdown policy. Our hospitals have been full for about 1.5 months now. We've been world leaders in daily deaths for probably a month or so.
Yeah, so the article after just saying that the lockdowns don't do anything, because all countries seem to behave the same, concludes with "well, we certainly need to explain this..." (they seem to read my mind). And then say nothing about it. But they have included this (just to contradict you): "Certainly, a full complete lockdown reduces the spread of the virus."
People forget, that epidemiology is a well established field of science. It's only new for them. If I'd have to guess why the epidemic could start to decline on its own, I'd say that people just shit in their pants after a while and start to keep more distance. This could probably be seen in the mobile tracking data if anyone cared.
The sad thing about the lockdowns and the restrictions is that they work pretty well. If combined with all the other efforts and if people comply. Because in the end that's what matters: what people do. Not what governments say they should do. If you (or any of those authors) care to look at East Asia, Australia and New Zealand, you'd see that it can indeed be controlled pretty efficiently. Not for free, but for a lot cheaper than what most of the Western world ended up with. What they do is the complete opposite of what we're doing and what you re suggesting. Instead of ignoring, they react very quickly and vigorously. Closing entire counties if they found a few infected (that's e.g. what I've heard from a guy living in Thailand - they have 70 dead for 70M). And this allows them to have less restrictions overall. Because math. You can stop it when it's just a very low number or you can fuck around and stop it when you have a lot of dead people, when your hospitals are full. Of course, if you can stop it by testing, contact tracing, light restrictions (no mass gatherings), masks, etc., all the better.
Another piece of interesting (but not unexpected) information is that the economic effects indeed correlate with the number of deaths. [1]
> If you want to continue killing tens of millions per year so you can save the lives of far fewer, you have no standing. Frankly, that position disgusts me.
I don't kill anyone, but you definitely look angry and seem to handle this on an emotional level. Which I get, a lot of people do this but it doesn't help with having a logical argument.
You've linked to two sites that aggregate data, and provided armchair analysis of them to back up your position.
I've linked to 30+ studies supporting mine, none of which you've mentioned or shown studies that counter them (I'd expect at least 10's of counter studies if you have any kind of a point, hundreds if it has merit deserving of such servitude).
Your examples of lockdowns "working" are East Asia, Australia and New Zealand. Firstly, most of East Asia actually did comparatively little versus the West, especially early on - when they were at the epicentre - and is hampered in implementing lockdowns by a significantly higher population density, and in general, in the case of Japan, a significantly older population, placing them at an immediate disadvantage at that outset.
Your other examples of Australia and New Zealand are poor. If anything is prone to be an outlier, and worthy of less consideration versus other countries, it's these two. Especially New Zealand. It's one of the most isolated countries on the planet, has a tiny population and little through traffic. Compare numbers against any other pandemic (eg, Swine Flu 2009), and you'll see it's always going to do well just fine regardless of what measures may or may not be employed.
Considering the well-established link between the sun and the proliferation of these kinds of viruses (ie, a "flu season"), which happens for a variety of reasons (not least is Vit D production), nullifies those countries as useful controls, particularly against Europe and North America.
Finally, we have the figure of 9 million people who starve, and 8 million people who smoke, both of which are preventable, and both of which could be solved which much less effort, less expense and less social cost, and these are just two - but you still wish to persist in saving the lives of considerably fewer, the bulk of whom were already near death anyway.
None of your arguments make logical sense, and you are unable to back them up with science.
Further, you haven't bothered to even attempt to refute my core logical arguments or the bulk of science I've presented to back them up.
I'm not learning anything from this conversation, but thank you for your engagement. Go well.
You're mostly repeating the claims of GP and I have already responded to these. Esp. this one: "Vaccines typically take several years of testing before being approved."
The so called long-term effects have been mostly non-existent with any vaccine. First of all, the very expression "long-term effects" is vague. Do we mean effects that only materialize over the long term (i.e. a long time after being administered) or effects that last for a long time? The latter can be known (well, with a worst case estimation) even with short testing.
And as far as I am aware, there is very little evidence of the former happening with former vaccines. I.e. the vaccine inducing some systemic change in your body that remains undetectable for years.
> If they truly believed these were safe and of tremendously important benefit, they could stand
> up and say "we accept responsibility for negative outcomes in accordance with
> ordinarily approved medication, and waive our rights to emergency use protections".
First of all who? You seem to mingle several groups into one here. It's not the pharma companies who believe that that these are very important, but the society. (Well, at least the ones who don't live in denial.) The importance stems from the seriousness of the epidemic.
And safety is not a binary/boolean attribute. Safety can be measured and the accuracy of the measurement has a confidence (i.e. a probability that it's within the estimated limits). Now the claim is that this measured safety is way above the safety of contracting COVID. And this is the very reason we know that it's beneficial. For the society. It's pretty clear that pharma companies don't make nearly as much profit as much it is beneficial for the individual countries. Just try to add up the cost of the lockdowns e.g. for a year and then devide it by the number of doses and see how much they should cost if calculated like that. You know what, let me do the math for you: a year of lockdown has been estimated to cost 251bn GBP for the UK[1]. The UK has 66M population. Let's calculate with 266M doses. That would give you 19GBP/dose (~26USD) for the vaccines per dose. Per year. But they won't vaccinate everyone, 80% would already be an over estimation (which would increase the value of price/dose to 32.5GBP and we're not just talking about money we're also talking about lost lives and a lot of frustration, which would further increase the value of these shots.
Comprared to that, the AstraZeneca costs about 2USD, IIRC, the EU pays about 16EUR (14GBP) for the Pfizer/Biontech one.
So it's not that the tremendous value gets all snatched up by the pharma companies. Also, they do have a responsibility. In the US they have been waived, but not in the EU. And guess what: a lot of people keeps saying the same things over here. (Including* that they don't take responsibility.)
The reason the US waived these companies is exactly because the vaccines are so important and valuable for the sate (i.e. for the people). A quick rollout was more important for them, than for the pharma companies. As a side note: some politicians over here (EU) think that the US did it the right way by not wasting time on negotiating hard with the pharma companies and that the EU is behind exactly because of that and that we should have waived them as well. (I'm not sure I buy into it.) But the EU non-waiver is an assurance for everyone else, including the US citizens. Yes, you may not get a million $ check if you happen to be unlucky, but it still shows that the companies indeed do have the confidence in their product you were talking about.
Resorting to calling people "anti-science" is just as counterproductive and unnecessary as calling them "anti-vax". You're only solidifying animosity and mistrust. People have every right to question what they're being told by the same governments who mishandled this epidemic from the start - especially since there such strong political incentives that aren't necessarily aligned with scientifically based recommendations.
Everything should start from a place of questioning. If there is data and the data makes sense, that can replace questioning with certainty. But often the data has a limited or tenuous connection, possibly even a fraudulent connection. This is why it’s important to actually read the studies and understand the science, not just to hand wave it away as “evidence = value.”
The technology behind this vaccine has been actively worked on for over a decade. Yes, these vaccines have been sent to market faster than normal, but they certainly have not been "rushed".
I hear this line being trotted out all over - especially from the "experts" - and I find it nothing short of enraging. There is a difference between saying "an mRNA platform in general might not be safe" and the actual claim real people make which is "this specific vaccine has not existed for more than a year and is being hastily rolled out on the world population via implicit or explicit coercion". The mRNA platform in general can be safe and, say, the Moderna vax could still have a poor safety profile. This is why we perform rigorous long-term testing and why most vaccine approvals (not that these are FDA approved of course) take several years.
If you can't be intellectually honest enough to admit that there is a difference between "we've used this platform in theoretical research in small numbers" to "we mass-market and roll out this novel vaccine to billions of humans worldwide", you shouldn't be in the discussion, IMO.
It's the same thing with flu vaccines, mind you. They only get a few months testing before entering mass use
The speed of access for these vaccines is that they started mass production while testing was ongoing, rather than waiting until after testing to start production
Thanks for the important clarification; I didn't read closely enough.
My argument was definitely tailored for the mRNA discussion, although the purpose was more to illustrate the broader principle, but, not knowing a whole lot about adenovirus vector vaccines specifically, is it even the case that adenovirus-vector vaccines have been widely used in the general population?
I couldn't find great info with a cursory search (indeed the top result is the CDC which consistently fails to cite anything they ever claim, ugh), but I wonder if the general argument still applies for these types of vaccines as well.
Anyway, thanks so much for catching and pointing out my error there.
> fwiw, new and better better technologies need to get used for the first time, eventually.
No-one disputed that, I'm just pointing out that it is a very valid point for someone to say "I have concerns that we're rushing out an experimental vaccine". You might take issue with the specific wording (I don't) but the general point I hope we can agree on.
It's not dishonest. It's a very adequate answer to the over-simplifying claim above. I.e. there is a difference between a newer and an older platform and there is a difference between an experimental platform and a new platform (that's not experimental but has been in development for a long time).
You can always argue for making things slower and experiments longer, the problem is, that there is a pandemic going on with 3M deaths in the past year. Actually people seem to think that you can develop vaccines without being rushed, but it doesn't seem to be the case. There are several reasons why other vaccines took years:
- it was a long time ago and scientists had a lot less knowledge, experience and older technology. (Think e.g. the mRNA vaccines, which J&J is not one of, where the first candidate could be completed in something like 2 weeks after the isolation and sequencing of the virus.)
- they had to start from 0 for a new virus (because they new less, etc.). Like for the polio, or HIV. In the case of SARS-CoV2, they could build a lot on the experiments from SARS-CoV1. As far as I know, there was a vaccine candidate back in 2003, but by the time it would go into phase-3, the epidemic was over. Also, it seems that research never stopped about the coronavirus vaccines, so there were new results between 2003 and 2020 that the mRNA vaccines built on.
- some viruses are easier to develop a vaccine for. (E.g. the HIV is not one of them, because it's very good at evading the immune system)
- I've already mentioned this, but if the vaccine candidate doesn't get ready on time because of the above reasons, then you may have to wait for years before you can do a phase3 trial because there will be no people getting infected, so you won't be able to measure the effectiveness. This is what happened with the ebola vaccine in 2014. Now the vaccine is 7 years old, but it doesn't make it any safer, because there weren't people who could be vaccinated. (Well, of course, you could vaccinate them and wait for any long term side effect, just in case, that would show up without being infected, but that doesn't seem like a very important data point.)
But again: why would you want to wait for several years in a situation like this when we do have a pretty clear picture of both the worst case risks of the vaccines and the risks of the disease (which are higher than the worst case risks of the vaccines).
> It's not dishonest. It's a very adequate answer to the over-simplifying claim above.
I would disagree that calling it "rushed, experimental, and not necessary for [the original commenter]" is an over-simplifying claim. Indeed I find the "we've done theoretical research with platform X for years" to be the oversimplification. That being said I do agree that there is a difference between an experimental platform and a new platform.
> But again: why would you want to wait for several years in a situation like this when we do have a pretty clear picture of both the worst case risks of the vaccines and the risks of the disease (which are higher than the worst case risks of the vaccines).
Starting with the "higher than the worst case risks of the vaccines" part, FWIW, this is true in general but not for all individuals. For someone like me (20's, active, no major health conditions), the acute side effects of getting a SARS-2 vaccine far outpace the expected level of symptoms from SARS-2 infection itself. (Speaking from a personal risk reduction standpoint only, I don't want to get into the ethics of medical collectivism for the purposes of this discussion). I don't think you would dispute that, but just wanted to mention it because it's because taboo (and indeed you can get actively censored) to say "for my specific health circumstance the vaccine is more dangerous to me".
As for the more general point about understanding the risks of the vaccines and the disease fairly clearly, I would say that we understand the virus far better than the vaccines. Indeed it really saddens me how we've wasted public health dollars on messaging to people that immunity to reinfection is not a thing (when it is most definitely a thing) and to be super spooked about variants despite the fact that SARS-2 is not going to magically mutate away from the spike protein anytime soon (i.e. there's plenty of epitopes for our immune system to work with even for the highly artificial immunity produced by making the body's cells manufacture spike protein exclusively).
I will grant though that we have bounds on how bad short or medium-term adverse reactions could be to the vaccines. Personally I worry less about the (using mRNA as an example here to illustrate a general point) "it's going to turn me into a human GMO" pseudo-argument than I do things like (a) "is the rate at which spike proteins get produced in the body much more of a steep increase followed by a steep dropoff leading to greater potential for acute inflammatory episodes than via naturalistic infection" as well as (b) "could we be over-sentitizing the immune system to react too strongly when it detects spike protein, particularly for those who already had COVID-19 before ever getting the vaccine". If you're not aware, an absurd amount of people who have already gotten COVID-19 and therefore have naturalistic immunity are still getting the vaccine, either because they're "required" to (aka they don't know or want to fight their job's requirements) or more often because they've been brainwashed to think that the variants evade natural immunity which is just a total media-propagated falsehood.
> In the case of SARS-CoV2, they could build a lot on the experiments from SARS-CoV1
Totally agreed and I wish more people knew that the virus causes COVID-19 is called SARS-2 and that it is directly related to SARS-1 (I'm referring to layfolk here). As a separate tangent I wish more people understood that the emergence of SARS-2 means we don't really need to worry about SARS-1 anymore because anyone exposed to SARS-2 will be cross-reactive with SARS-1.
> I've already mentioned this, but if the vaccine candidate doesn't get ready on time because of the above reasons, then you may have to wait for years before you can do a phase3 trial because there will be no people getting infected, so you won't be able to measure the effectiveness.
This is simply not the case for an endemic seasonal respiratory virus. You'll have plenty of cases, especially since we're basically PCR-testing the whole globe (I don't think we should be, to be clear). But I totally agree that the apparent benefit of vaccines declines exponentially as time goes on, particularly with SARS-2 where the fact that it is deadly for the very elderly and harmless for the very young means that yearly recurring mortality is going to essentially vanish after it's propagated through the current world population (as an aside, this fact is one of many reasons why all the hysteria around the virus was absurd from the get-go; amortized over several years the mortality of SARS-2 is entirely unremarkable)
> But again: why would you want to wait for several years in a situation like this when we do have a pretty clear picture of both the worst case risks of the vaccines and the risks of the disease (which are higher than the worst case risks of the vaccines).
Yeah, to conclude I want to bring it back to my earlier point which is that once the virus has propagated through the current world population (more or less), the set of SARS-2-naive individuals will become dominated by the very young, who are not at real risk of COVID-19 and therefore they will develop immunological memory while young when they are incapable of being harmed by SARS-2. This means that recurring yearly mortality will fall off a cliff (albeit, if we keep labelling deaths the way we do we won't see that reflected in the numbers nearly as much as we should). Which is why I think the restrictions and everything else, even if they had worked in places like the US or Europe where they totally failed, were always a bad idea. But the other side of that coin is: yes, insofar as you do think SARS-2 is something worth really freaking out over, we absolutely have to rush the vaccines because if we wait 2 years then there won't be any real COVID-19 deaths left to mitigate.
They slapped the word "experimental" on the disclosure form and waived liability to the manufacturer... it was rushed... as it should be. I took it. But the reason people don't "trust the science" is that its obvious people are lied to on a regular basis around covid and trust has flatlined.
> Agreed, I've had all other vaccines, but this batch is rushed, experimental, and not necessary for me - labelling people such as myself "anti-vaxers" is just dishonest, bitter, childish, name calling.
No, it's not. That's a misunderstanding of how the vaccine development process works and what takes time.
What takes time in the normal course of development is testing the vaccine, yes. Specifically, determining how effective it is. The reason that takes so long is that in general there are very, very few cases of most of the diseases vaccines are developed to prevent -- and you can't just go giving people Ebola to check how many of them catch it.
It's fearmongering, plain and simple.
There's mountains of data for your perusal online explaining how and why it got done fast -- here's one example. [1]
Nine women cannot work together to produce a baby in one month.
Similarly, while wider population testing for safety and efficacy would likely correlate with long term safety, it’s not a total substitute.
I think it could be completely rational for young, healthy, low BMI people to delay vaccination till they’re more comfortable with any potential long term issues.
Well I guess it's a good thing nobody's trying to produce a baby, but rather, a vaccine. Because they succeeded, and you hand-waved away my completely rational explanation with a nonsequitur about pregnancy.
Those folks aren't being immunized to protect themselves but those around them. This is a team effort and everyone's gotta pitch in.
> I think it is a disservice to outright label people as anti-vaxers simply for questioning the risk-calculus of vaccines.
It's the same idea though, and should still be called out. It's people who have unqualified medical opinions, and who are then often spreading that opinion to others as if it's useful.
Let the agencies figure it out, pay attention to the latest recommendations from them, and go with that. Anything else is just the blind leading the blind and should be called out.
Careful to not play the appeal to authority. Anyone can understand anything, regardless of their so-called qualifications. Are they likely to? No, and that’s why someone’s qualifications are purely a heuristic, not a prerequisite.
It's extra frustrating because organizations like the CDC get held to lower standards than anyone else. They can make a pronouncement recommending the use of face masks for SARS-CoV-2 community transmission when the body of the research confirms that (a) such intervention has never been tried in an RCT and indeed the whole "my mask protects you" hypothesis is intentionally unfalsifiable, (b) the research literature documents numerous negative impacts whereas the positive impact on transmission is completely unproven at best, and yet their evidence-less pronouncement is considered evidence in its own right and such a pronouncement is used as a citation in Wikipedia articles, etc.
(Just using masking as an example, if any onlookers strongly believe that masking is efficacious for the stated purpose just imagine I gave a different example, although I don't see how anyone could reach that conclusion about masking specifically based on the research literature out there which is neutral at best)
Or as another example, the CDC loves to try to encourage people to take the flu vaccine, and yet I was shocked to discover that it takes 71 flu shots to prevent a single flu case, 29 flu shots to prevent one ILI (this is a better number than the flu case number since really we care about ILI in general, but even so 29 is an abysmal number), AND that regardless of the mediocre reduction in cases/ILI, it makes essentially no difference in hospitalizations.
I didn't realize until this year how much of "public health" involves (a) actively and intentionally lying to the public (for example, if you read about the AIDS crisis you learn about the "noble lies" told about who was vulnerable as well as the not-even-noble lies like when Fauci told people you could get AIDS from close contact with someone with AIDS when the scientific evidence showed that to be false), and (b) is really a giant marketing campaign for various big pharma interests (I say that as someone who is an unashamed free-market capitalist, not that the US is actually a true free market when it comes to the pharma/medical industry)
I'm not insisting that a claim is true just because an authority says it is. You can't just bring up "appeal to authority" and call it a day.
I'm insisting that the average unqualified individual should not think they have a better chance of being correct over the authorities in question.
There's no other rational option for unqualified individuals than to listen to medical authorities unless you have a medical degree yourself and have read and analyzed the research yourself.
There are actually a lot of reasons to be skeptical of experts — the same as why you should be skeptical of anyone. Appeal to authority has a contrapositive: the disappeal to lack of authority. The arbitrary person can be right just as much as the expert can. The whole point of logic and reason is that it’s about facts, not the people.
Critically the problem with your reasoning is the last sentence. No, you do not need to have a medical degree to be right when a doctor is wrong; ask anyone who’s had a medical issue that all doctors agree does not exist.
True, the word was wrong. The point though is that for this logical fallacy, there is an equal and opposite logical fallacy. Saying authority implies truth is just as wrong as saying lack of authority implies falsehood.
How does authorities being wrong / changing their recommendations factor in to what your consider a rational option? If you were a high risk individual back in January 2020 who ignored their advice and quarantined + wore a mask (an effective mask, i.e N-95), you made the right choice.
Despite how much smarter and informed humanity is, we still make decisions based on trust. Science can only explain so much and runs out of answers eventually.
> If you were a high risk individual back in January 2020 who ignored their advice and quarantined + wore a mask (an effective mask, i.e N-95), you made the right choice.
Did they? Or was the chance they'd come in contact with Covid at that point very low and those masks would be of much better use at hospitals where the chance of coming into contact with Covid was very high? At least, that was what the experts were saying at the time. I donated my N-95 masks (that I had from California fires) not because we thought they didn't do anything in January 2020, but because the experts said they were of better use in hospitals.
> Science can only explain so much and runs out of answers eventually.
You say this as if there's a better place to find answers. Where is that place?
> Did they? Or was the chance they'd come in contact with Covid at that point very low and those masks would be of much better use at hospitals where the chance of coming into contact with Covid was very high? At least, that was what the experts were saying at the time. I donated my N-95 masks (that I had from California fires) not because we thought they didn't do anything in January 2020, but because the experts said they were of better use in hospitals.
You're saying a high risk person (high risk meaning they would likely die from covid - immunosuppressed, etc.) wearing an N95 mask and quarantining was a bad choice? I'm not sure how those masks would be better used if the person is at a high risk of dying to covid.
> You say this as if there's a better place to find answers. Where is that place?
Interpreting all the data available to you. Would you have shamed a person for not choosing this man as their surgeon https://en.wikipedia.org/wiki/Christopher_Duntsch after they researched his past operations. There are more factors than just the research that need to be considered.
In 2012 if someone decided against their doctor's advice not to take an opioid which the FDA had greenlit as safe in far too many cases, would you call that "blind leading the blind"?
Iatrogenesis rivals strokes as a cause of death. Most doctors are just slavishly following official doctrines from authorities, and sometimes those authorities get it wrong. We don't even have to look to the Before Covid Times to see examples!
Yes. That's correct. That doesn't change what I said.
Answer me this: why do you think unqualified individuals are better suited to get it right?
Just because there are examples in the past of people who went against the recommendations who ended up being right, doesn't mean you should take everything else into your own hands. Unless, of course, it's literally your job.
It’s not a question of getting it right, really. I haven’t heard a single uneducated opinion say, “You should not get it because X”. I’ve seen several say, “I will not get it because X”
It’s a subtle, but IMO important distinction. If people wanna rationalize not getting the shot based on their own misunderstanding of the science, that’s fine. That’s okay.
We don’t need universal understanding here for the vaccine to do it’s thing. Let those who want to get it, get it. And those who don’t, to not get it.
> I haven’t heard a single uneducated opinion say, “You should not get it because X”.
It's not even 3 hours into my day and I've already received 3 texts from family saying something along those lines regarding J&J, even if it gets unpaused. It's a much more prevalent thing to say than you think.
> If people wanna rationalize not getting the shot based on their own misunderstanding of the science, that’s fine. That’s okay.
It's not okay. We need shots in arms. And you're doing your part by enabling those who are misunderstanding the science by making them feel like it's okay to not get the shot.
Deciding that your pain is well managed without opiates has always been a perfectly reasonable and medically-accepted option, and unsurprisingly there has never been any sort of social stigma against people who decline painkillers.
Most to the point, declining to take painkillers does not adversely impact other people's health.
This is not a good analogy.
eta: ironically, the problem with the opioid crisis was not too much regulation and oversight by "the authorities", but too little; too much freedom for doctors to prescribe stronger painkillers, and for patients to request them.
I agree that, unless you have specific concrete reasons to think a public health agency is distorting the facts or making decisions based on politics and ass-covering instead of optimizing for health, you should trust that agency. However, once you have concrete reasons to think that the public health agency is acting on politics and not science, you should not continue to blindly trust them.
There are other sources of information besides the public health agency of your particular country, for example public health agencies in other countries, or directly looking at the stats and research papers. In this case, looking at the stats makes it blatantly obvious that your risk from the J&J vaccine is much, much lower than your risk from getting COVID, so if your choice is "J&J" or "no vaccine for another month or two", you should probably pick J&J.
> I've already seen a bunch of anit-vaxers referring to this
It's not only a disservice, it's a biased way of thinking which only serves the one making the statement, given it allows them a way to alleviate their concerns about having received a level of uncertainty from their actions. I get them them because I also got that shot!
The problem isn't 7 out of 7 million odds. It is that it is an unknown side effect that did not come up in the original studies.
We have approved vaccines with worse side effects before. The difference is that we knew what those side effects were and weighed the risk vs reward and made the call to use it.
> an unknown side effect that did not come up in the original studies.
You shouldn't expect side-effects this rare to show up in the trials. The AZ trial was based on ~32k participants (https://www.astrazeneca.com/media-centre/press-releases/2021...). Your probability of observing a 1/1,000,000 occurrence in 32k observations is something like 3%.
It's impossible to uncover (with statistical significance) 1/1,000,000 side effects without giving millions of doses.
The fact that a rare side-effect has (maybe!) shown up should not negatively impact your priors for how safe the vaccine is. If anything, the fact that we're talking about 7 / 7,000,000 cases should reassure you that we're catching extremely rare stuff, which means we would have caught anything more serious too.
A more general way of putting this is that, by doing a trial you don't prove there are _no_ side-effects, you just put an upper bound on how common they can be. This is the best that science can do! Epistemologically speaking, you can never prove the non-existence of something, you can just show that it doesn't occur in the places you've taken measurements, at a frequency that your experiments would detect. (This is the "black swan fallacy", as John Stuart Mill originally formulated it.)
Yeah and we only just started to roll this vaccine out - so it's fair to say that the risk will likely grow beyond that.
You're right that 7 / 7,000,000 are good odds, and most people would likely take them - but it would be unwise to not give people an educated choice between vaccines if there are known risks.
> but it would be unwise to not give people an educated choice between vaccines if there are known risks
They are not giving people an educated choice, they are taking that choice away until they deem it okay to give it back. Education is knowing that 7/7,000,000 had a blood clot + the other tests that were done leading up to its release. We know that now. We're educated.
It is CVST not just blood clots. There are a lot more blood clots with or without the vaccine. CVST is rare so is the proverbial canary in the coal mine here.
The CVST incidents give a lower bound on risk. The trial data give a rough upper bound on risk (rough due to the small sample size). Knowledge is being refined here. We can't make educated choices without knowledge.
Hard to give people an educated choice without looking into the issue first. Once they know what is going on it will most likely be back to normal. There was a similar issue in Europe, but that neatly overlapped with a delivery shortage of the affected vaccine.
It is impossible to rule out unknown side effects. The blood clots are now known. Any side effect that is unknown will always remain unknown. You could always be the first person to experience a symptom, whether it's Tylenol or this vaccine.
> All six cases were in women aged between 18 and 48, with symptoms appearing six to 13 days after vaccination.
Presumably, some of the 7 million people who have gotten the vaccine did so in the prior 5-12 days. It is reasonable to expect to see more cases over the next 6-13 days from the moment we pause J&J vaccination.
Also, if the effected group is only young women, the denominator isn't really the same as the total number vaccinated. Not saying it isn't still very rare, but in young people COVID deaths are also very rare. We have alternative vaccines, it makes perfect sense to advise young women against J&J for the time being while this is sorted out.
And for anyone that thinks this is just normal incidence of blood clots being blamed on the vaccine - that's what was said about AstraZeneca originally, and if these clots are anything like those it is absolutely not the case. Those are serious clots that are very rare to see period, let alone in young people, and require different treatment than normal clots (they have surprisingly low platelet count).
I suspect US agencies had good reason to want to pause J&J given all of that - the AZ vaccine issues were also disproportionately affecting women interestingly.
I guess I wasn't being specific - good correction. Reporting medical side effects can easily lag with new treatments, especially when we're not sure what we're looking for.
I suspect that, as soon as we start looking for blood clotting post-vaccine, then you'll find more cases that may have not been caught otherwise due to their not being severe enough to be noticed.
This exact thing happened with the AstraZeneca vaccine, which works very similarly to J&J. The EMA is now recognizing thrombocytopenia (not the same fatal issue but possibly related) as a "common" side effect, i.e. somewhere between 1 in 10 to 1 in 100.
Provided a larger sample size, doesn’t an increasing rate of an outcome suggest existence a confounding variable that the smaller previously tested sample failed to identify, and (not absolutely- but more likely than not) would apply increasingly at the larger scale? Not a statistician here- and honestly asking.
Lets say these side effects only happen in certain populations.
If that is the case we could then target this vaccine to the rest and have it be much safer while giving out the Pfizer-BioNTech or Moderna vaccines to this group.
End result is everyone still getting their vaccine fast but less side effects (and possibly deaths due to worst case side effects). This is why we need more data or the time to study the data in this case most likely
Agreed. Another unknown is how many people may have had some clotting issues that were mild and unreported. As you note, even though the 7/7M odds are compelling, the effect is still unexpected and there are two other vaccine alternatives. Taking a pause to consider the issues and perhaps make adjustments in suitable patient profiles and/or adjust follow up observation and early intervention treatment protocols for the issue makes sense.
Don't know if it matters to anyone, but the "FDA has suggested that health care providers pause the use of the vaccine while the side effects are being studied. However, providers are not prohibited from using the vaccine if they feel the benefits to an individual patient outweigh the risks." [1]
So we stop giving out treatment and an extra 1000-10000(?) people die and we delay the economy getting back on track for a week or two with the delay. No skin off the FDA bureaucrats teeth, but they are hurting a lot of people with this decision.
> It is that it is an unknown side effect that did not come up in the original studies.
It's not clear that this even has to do with the vaccine. If you gave 7 Million people a glass of water on the same day, I'm sure at least 7 of them would experience some sort of moderate to serious health outcome in the days that followed.
For young people (it seems especially young women) I think the answer could end up going in either direction honestly. I think it's completely reasonable to redirect them to mRNA vaccine until we know more.
Not sure why the J&J vaccine had to pause for older population where clearly the vaccine has a much better benefit/risk profile though. But at least in my area of the US the vaccination rate for senior citizens is quite high already.
"Doctors For COVID Ethics" a (non anti-vax) group of 150+ medical professionals/university professors etc, warned in March about the likelihood of deaths resultant from exactly this issue. They went public with their previously private correspondence with the European Medicines Agency, as they were unsatisfied with EMA's responses. Who picked up their pleas? Conspiracy, fringe and some right-wing websites - that seems to be it.
To be clear, we haven't determined that it's actually a side effect. That's why they've stopped, to get a better handle on what actually happened, and what to do about it.
It could be related to the vaccine, it could not be. It could be 1 in a million, it could be 1 in 100k.
Nobody has investigated 7 million doses, so its at least 7, but probably more. The UK incidence rate (for the same issue in the AZ vax) was like 10X what was initially reported.
And its probable that these incidents are concentrated in a small segment of the population (young & health maybe women). So your denominator is very inflated.
If you can save 20-40 lives by just giving young women Pfizer and using J&J on 50+ year olds (for whom the risk might be literally nothing) then its a no brainer.
Not doing so is killing 20-40 people for no reason.
Yes this is the rationale Canadian authorities have used in making AZ 55+ only here. Some calculation based on risk of COVID mortality in that population vs the hypothetical AZ risk. At first I was skeptical of this but the more I read about it the more it seems like a reasonable approach.
Even more so because here in Canada we do not have much AZ yet anyways (and no J&J yet), mostly Pfizer and Moderna.
They didn't pause it because they're considering cancelling it. They're pausing it so they can communicate to patients and providers what to look out for after they take it. Once processes are in place to handle future blood clot events, they will resume vaccinations.
I’ve been thinking about this, the communication has been so bad from public and private health officials for 15 months straight.
When not considering any externalities, anti-vaxxers and everyone that comes up with anti-industry and anti-establishment conclusions is rational, but inaccurate only because they dont consider what was not said.
Even with regard to COVID itself, most of the official communication is about avoiding death when the reality is that its not about only avoiding death its about all the additional debilitating effects in the vast “recovered” statistic, so it is rational to decide to ignore that once you do your own math and noticing who is actually dying. But it is not accurate because it doesn't factor in the unsaid aspect.
The reason for the pause was explicitly stated by the health officials as quoted in the article, so I don't know why you'd say this was unclear let alone unsaid.
They might also add additional guidelines for who is eligible for J&J. A bunch of countries have set a minimum age for AZ vaccine, I could see something similar happening here with J&J. Perhaps excluding women under 50 for example.
But I agree J&J will definitely resume in some capacity in the near-ish future.
Multiple advanced health care systems in the world are independently pulling these vaccines. I wouldn’t brush it off as the FDA being overly cautious. None of these vaccines have been tested in humans for more than 12 months. And you’re assuming that health authorities can wave a magic want and instantly know who is having some kind of undetected brain clotting? I think the risks are extremely unclear even though people are throwing statistics around like they mean anything.
Not a single one of those health authorities allowed vaccine challenge trials. That tells you how much they care about saving lives versus how much they care about not getting blamed for any deaths.
> The main benefit of challenge trials is to speed up development as I understand it not to broaden risk estimates.
Right, which is why it was crucial to have such trials a year ago. We could have shipped vaccines 3 months sooner and saved hundreds of thousands of lives.
Unfortunately, no health authority was willing to risk blame for any disabilities or deaths stemming from deliberately exposing consenting people to covid. So we had to use much larger sample sizes and wait longer to know which vaccine candidates were effective.
I believe their concern is more of long term effects and not short term. A vaccine isn't meant to cause blood clotting, unless we know the specific mechanism of how that's happening it could be much more dangerous.
No doctor or expert. But I did follow the AZ story. I understood, that Covid can cause blood cloths. A vaccine triggers an immune reaction, in that case Covid, so a particularly strong immune reaction, maybe together with a preposition of developing blood clots, can be a reason. Not sure if we know already what causes these side effects with AZ an JJ.
From a risk perspective, I wouldn't restrict either vaccine. But since we can easily use Moderna and BiontechPfizer instead for the most at risk groups it doesn't really change things, does it?
Most immune reactions will cause blood thickening. If your arteries are already full of crap they will clot, this is why if you are at risk of blood clots you need to be careful even when you get the common cold.
More to the point, they have temporarily paused because the usual treatment for blood clots can make this particular type of blood clot worse. So they are pausing to give the medical community enough lead time to get up to date on treatment protocols.
Vaccines are held to such a high standard. We wouldn't have approved even Aspirin if we applied the same standards.
If I have my numbers approximately right, getting the J&J vaccine is a bit safer than taking a plane trip, while getting COVID is about as safe as taking a trip in the space shuttle.
Your chance of dying from COVID is heavily dependent on your age and any preexisting conditions, so any comparison that uses a single probability for everyone is totally wrong for a very large number of people.
One person, out of the 6.8 million who have gotten the J&J vaccine, died from blood clots. A second is in critical condition.
Yes, your risk of dying from COVID varies with age, but not to that extent. Even among children, the death rate for COVID is an order of magnitude over the 0.000015% to 0.000030% chance of death it would have to be for the decision to stop using the J&J vaccine to make sense, based on the numbers we're making that decision based off of. Among the people who are actually being blocked from getting the J&J vaccine (e.g. mostly 20s/30s/40s adults), the decision looks much worse.
> Your chance of dying from COVID is heavily dependent on your age and any preexisting conditions, so any comparison that uses a single probability for everyone is totally wrong for a very large number of people.
It also depends on the rate of community spread (and what's spreading) in the communities you're in.
The exact same caveat can be made for people who are vulnerable to the extreme side effects of the J&J vaccine. It depends on specific characteristics of the person taking the vaccine. “any comparison that uses a single probability for everyone is totally wrong for a very large number of people.”
Yes, with the key point that the people who are most at risk of dying from the vaccine are a different set of people than those most at risk of dying from COVID.
> I've already seen a bunch of anit-vaxers referring to this in new articles this morning.
So, take pause and examine the situation. Are these people actually anti-vaxxers, ie they oppose all vaccination due to weird paranoia about autism due to a discredited "study". OR are they against this one vaccine because of political affiliation.
I'm really concerned that if we call out the people who are afraid of this one vaccine as anti-vaxxers that we'll only succeed in introducing them to the wider world of being afraid of all vaccines.
Find a different term so that we don't introduce these two groups of people to one another and give them a reason to join forces.
> OR are they against this one vaccine because of political affiliation.
It's not easily attributable to "political affiliation." Trump was touting the vaccines through his whole campaign and is still bragging and taking credit for them. MSNBC did one of those TV segments where they go and interview backwards people from America's hinterland who weren't planning to get vaccinated, and although most were Trump voters, not a single one said they would change their mind if he advocated taking it.
The actual difference between these vaccines and others which is driving skepticism is that we have no observational data about their long-term effects.
It goes beyond "radicalizing" potential anti-vaxxers IMO, because at this point it's become like its own religion, where every vaccine must be equally good and questioning a vaccine is somehow outrageous.
US agencies are the ones recommending a halt. US refused to approve AZ, and Europe halted it, in many countries imposing additional restrictions when resumed. Doctors specializing in the field agree these are legitimate concerns.
If people want to argue cost/benefit tradeoffs, or speculate on things we aren't sure about yet that's totally cool, as long as they are upfront about it. And I understand if someone still wants to get J&J and is upset or just generally disagrees with the total/forceful pause.
But I don't understand treating anyone that has a concern about J&J like a brainwashed neanderthal, when literally the actual medical community has reservations about this particular vaccine. As a young woman I would not get J&J right now. Luckily I was able to get Pfizer instead.
Anyway, I agree there is a problem more generally with scientific education that can push "moderately misinformed" people into much deeper rabbit holes instead of working to educate them. I guess my point is just that I think this is a good example of how people have gotten so entrenched in the issue that it has reached a new level. There will be cases when the science is legitimately unclear, but the popular sentiment will all of a suddenly decide "science says X" and then the internet runs with it.
Another example - there was an ~2 week period last March where I had multiple educated/"science supporting" friends talk down to anyone considering a mask. No it was not coming from a hoarding perspective and it had 0 sense of uncertainty about it. These were strongly worded statements about how "masks don't do anything for COVID, the science is pretty clear".
On the medical benefits alone it seems obvious to continue giving J&J. The counter-argument I understand is that J&J's supply is severely limited due to manufacturing problems right now, so pausing it doesn't significantly slow down the vaccine rollout. There are a lot of people right now that saw headlines about J&J's manufacturing defects, and now this one death, and are convinced those are related. Visibly pausing something that is such a small percentage of the vaccine rollout might be a good political move.
Full disclosure: I took the J&J vaccine last Thursday, and would do so again right now.
We usually test vaccines for a decade because of the risk of unknown short term and long term side effects. If we don't know why people are getting blood clots from the vaccine, then we don't understand the vaccine and could be creating long term issues for many people.
We don't. Vaccines are monitored, called phase 4 trials. Taking place after approval. No vaccine was tested for decades before approval. It is only that development and approval takes longer, in case of the Covid vaccines approval red tape was cut. And not trials.
It's not the risk of clots. It's the risk of vaccine hesitancy because people fear a cover up. I think that's outweighed by the increased vaccine hesitancy because people only hear this scary story and not the low numbers (see also AstroZeneca).
Unfortunately this "pause" will also result in vaccine hesitancy (on top of vaccination delays). We know this from the EU experience with the AstraZeneca vaccine which is now distrusted by many people.
This will almost certainly now be a problem with the J&J vaccine in the US. More people will get sick and die because of this.
You know, for all the continual fear mongering about coronavirus last year, the constant reminders of who was most at risk, the hyper importance put on masks and cleanliness, etc it is shocking to see things put this way now.
That's because long term consequences of COVID are real, and worrying just about the worst case (the death rate) is like saying that data leaks are no big deal because only 2% of them lead to the loss of their customer's life savings.
I am not so sure those long term effects (except those that lead to blood cloths) are real.
A quick duck duck go shows that these are the symptoms:
Tiredness or fatigue
Difficulty thinking or concentrating (sometimes referred to as “brain fog”)
Headache
Loss of smell or taste
Dizziness on standing
Fast-beating or pounding heart (also known as heart palpitations)
Chest pain
Difficulty breathing or shortness of breath
Cough
Joint or muscle pain
Depression or anxiety
Fever
Symptoms that get worse after physical or mental activities
Apart from the loss of smell, those are all things that are hard to quantify and could be something you are not aware of until you start looking for them. At which point you might become anexious and really start to notice them.
I’d probably be careful using this as a public health communication tool; you’re comparing these risks to things like flying, which people are viscerally afraid of. Not to mention that the CVST issue is a poorly understood and evolving picture, so it’s hard to confidently assert that the risk is actually a micromort.
The perceptive gap between zero risk and extremely small risk is enormous. If I’m young and healthy, I can easily avoid the additional 1 micromort risk of taking the vaccine by simply not taking it. Now what?
That is of course true, and you're free to weigh up the risks however you like. Also true that there are unknowns. But the benefits of the vaccine are known too, and the risks of COVID include death and long covid, which also has unknowns and does not look nice.
Let me try one more way I have been thinking about it. I'm also weighing up whether I should get the vaccine and TBH made this site as much for myself as anyone else.
The point of the site is really to show the fallacy of there currently being zero risk in your life. Comparing 'none' to 'additional' isn't really what is happening. You have risks in your life every day, every time you do anything.
On any given day you already have about 1 Micromort's chance of dying from any unnatural causes. So that's 365 a year. So getting that vaccine puts it up to 366.
That's an increase in risk of just under 0.3% for the year, from an already pretty low baseline of likelihood of dying that we enjoy these days.
This way of thinking helps me. I'm hoping it might help some others too.
I'm not sure where you're getting your stats, but so far I've gotten
> That's about 10 times less risky than walking down the stairs
and
> That’s the same risk as driving for 5 hours
Which implies that walking down some stairs is equivalently risky to driving for 50 hours. That seems... unlikely.
There are about 150 deaths per 10 billion passenger-miles in the US [1]. That means that a micromort (a 1 in a million chance of death) corresponds to about 66 miles driven, which would probably be about 2 hours of driving.
In 2000, 1,307 people died from falling down stairs[2]. The US population in 2000 was about 280 million, so 1307 / 280e6 / 365 = 1.27e-8, so the average person had about a 12.7 in 1 billion chance of dying by falling down stairs on a given day. It seems reasonable to estimate that on average, each American goes down stairs about once per day (some people never go down stairs, others go down them multiple times per day). As such, I think the estimate for "risk of going down the stairs" should be more like 10 in a billion and less like 10 in a million.
Hey thanks for this. I have the sources next to each. Just click the link in the bottom left corner. Let me know if you don't think they're accurate after having a look.
I took the driving risk as being 250 miles of driving with an average 50mph speed (The risk of dying must be higher at high speed so wanted to take a high average to be fair).
The source on the "10x less risky than going down a flight of stairs" is https://static.guim.co.uk/sys-images/Guardian/Pix/pictures/2.... That shows that in the UK in 2010, 655 people died from falling down stairs. That translates to a 1 in 100,000 annualized risk from falling down stairs -- the relevant comparison is "10x less risky than using stairs a typical amount for an entire year".
Interestingly, running the numbers for the UK shows that the annualized per-capita risk of dying on stairs in the UK is more than twice as high as it is in the US.
Thanks. I'm going to take that one out. Makes it simpler not to do annual risk. Risk difference UK/US is odd! We thought you guys had it bad with gun crime, and didn't think about the stairs....
This is brilliant, I manage IT systems for hospitals and clinics and hear the front desk staff using analogies like this to put the risk into perspective. For something like this it shouldn't matter if you're even an order of magnitude off, the point is to help the non-mathematically-inclined general population understand how low the risks are in a context they understand (and anecdotally I'd say this strategy works well).
This is true, but I find it funny and frustrating that people are so ready to selectively treat rare odds as catastrophic in other circumstances that suit their worldview. For example, urbanists are ready to accept the premise of Vision Zero, which aims to push road fatalities down to zero. Today, there is approximately 1 traffic fatality per 100 million miles traveled in the US. It's so rare that it doesn't deserve attention, but here we are, with people looking to force cars to drive slowly (or ban them outright) to try and chase a world with perfect risk-free conditions. I am betting the same cohort that supports Vision Zero overlaps significantly with the group that thinks none of these vaccines should be paused. I'm sure there are similar examples of logical inconsistency that we can highlight for any political/social cohort as well - that's just one example. But my point is people tend to selectively make data driven arguments only when it suits them.
I don't get your logic? I would have thought people supporting project zero - essentially believing there should be zero risk to any individual at society's expense (having to drive slow) would want the vaccine paused for the same reason. To save individuals from getting a blood clot at the expense of society not being able to reopen.
I think there is another relevant part to it. I’m probably on the cusp of risk between Covid and vaccine at 39. But getting the vaccine stops it spreading and protects other people and will generally help the would and country get back to normal. So I’ll get the vaccine as soon as it’s offered to me.
I'm not sure about under 30, but if you take natural causes out of it, you have around about the same chance of dying today - check out 'the micromort' for more details!
It could be that the side effect has delayed onset, so there could be many people out there who are about to have the side effect but haven't showed up in stats yet. In that case I think it makes sense to pause for a while and wait for updated numbers
"The MHRA said about four people in a million would normally be expected to develop this particular kind of blood clot - though the fact they are so rare makes the usual rate hard to estimate."
That was my first thought as well. However, both vaccines with this issue are viral vector vaccines. Might be coincidence of course, but it gives me pause.
You are mixing certain numbers. It absolutely makes sense for my grandfather to get any vaccine, because of his risk, but the age braket for me means that I am more at risk of dying from Astra-Zeneca than Covid, but I am also a man and those who have died so far have been women.
I haven't seen enough numbers for J and J, but you have to untangle the various risk factors before you can say anything about what you should do as an individual.
I know this pandemic is fustrating as hell, but if you call people who use science and numbers to see problems with the current vaccines anti-vaxers then you will be taken as seriously as you deserve.
7 people in a fairly specific demographic (women 18-38, I believe), when there are 2 other alternative vaccinations available.
Do we have any data on the total number of women 18-38 who received this vaccine? It may actually be fairly low given we may have selection bias to give these vaccines to an older population.
The outcome may simply be to recommend that members in this demographic avoid this particular vaccine until further analysis is done.
Though rates of increasing the risk of blood clots for different birth controls vary, the ones that do range from 2-6x. The FDA estimates that in US out of every 10 thousand women using combination oral contraceptives or birth control pills 3 to 9 will develop blood clots each year while for comparison the same rate for women who are not pregnant and do not take COCs is 1 to 5 which is interesting considering the age range of the six cases.
That said research is beginning to understand the mechanism of these rare blood clots in connection to adenovirus vector meds and since it is so rare it's hard to get a precise number but other studies predict an excess increase of severe blood clots in the range of 1 in every 500 thousand to million patients.
I think that's not a very charitable take on "anti-vaxers". People are against injecting something new that has not stood the test of time. We have no idea what the actual frequency of this issue is (maybe more reports will come in), or if there are other lurking side effects waiting to be observed as a pattern, or if there are long-term effects. What if news of this spurs others to make the connection with the J&J vaccine and more such cases are reported to the CDC? Or looking at the other vaccines, what if in 30 years we somehow establish a link between mRNA vaccines and cancer?
I'm sure people will be tempted to jump in here and state their case as to why certain long term effects are not possible, and why this is conspiracy theory misinformation. But that's not the point. The reality is that humans regularly fail to understand infrequent or long-term consequences of new innovations, despite the best of intentions and despite the use of the best science available at the time. This has happened repeatedly in the past - see numerous prescription drugs that were recalled, or the use of phthalates in shampoos, or asbestos, or whatever else.
In the case of J&J, consider that this is happening against a backdrop of a continuously changing story about the AstraZeneca vaccine, increasing reports of COVID vaccines affecting menstruation (https://vajenda.substack.com/p/the-covid-19-vaccine-and-mens...), and a rushed emergency use authorization process that bypasses typical methodology for approvals of vaccines. The comparison isn't between the IFR of COVID-19 and the fatality rate associated with this vaccine. It's between the IFR of COVID-19, which is known to be very low, and the unbounded potential of near-term or long-term fatality or other side effects from the vaccine.
In addition, I'm very concerned that if we call people afraid of the covid vaccines anti-vaxxers that they will decide to join forces with real anti-vaxxers.
I know several people who are not interested in covid vaccines for what as far as I can tell are political reasons (although there are a few concerns about using a new technology before long term studies are performed). Right now they aren't anti-vaxxers. They get vaccines and they get their children vaccinated. It's just the new covid ones that they're hesitant about.
If we just lump them in with anti-vaxxers then they might decide to go make friends with the real anti-vaxxers. And as a big of a problem as covid has been, I'm more concerned about polio making a comeback tour.
I am not concerned with impossible to predict future events, but all effective vacines[0] will cause cancer in that they prevent people from dying early and so make it more likely they get cancer.
> oh and is 100% effective at stopping you from dying. Literally no one that has received the vaccine has died from COVID19.
This is misinformation (and I call it that because it is being widely repeated in major new sources). It's an improper generalization from what was observed in a very small sample of confirmed Covid cases in the vaccine trials.
>So far, more than 74 million people have gotten fully vaccinated in the United States. It's unclear how many have later gotten infected with the coronavirus anyway. But Michigan, Washington and other states have reported hundreds of cases. Most people have gotten only mildly ill, but some have gotten very sick. Some have even died.
This really is a sad, sobering reality. "6 cases in 6.8 million", ~0.00000089% chance of death via J&J vaccination. Extremely disheartening to see, but rather telling, where priorities lie. Politics aside, this is sheer stupidity, as you mentioned. Brace for another year as mutations continue to develop throughout the developing world while we waffle over infinitesimally minimal risk.
>Vaccination is also about stopping the overall spread of infections.
Then why are people still asked to wear masks in stores even if they are vaccinated? I've heard from the media non-stop that even if you have the vaccination you need to wear a mask - it doesn't make sense.
a) it's not entirely whether vaccinated people can still be carriers. I think it's now /mostly/ clear that they don't.
b) people are fscking awful. If you let vaccinated people not wear masks, you're going to have a bunch of philosophical zombies lying about their vaccination status to avoid wearing masks in public spaces. So, everybody wears masks until this thing is over and then some.
> All these anti-vaxers talking about living in fear of a virus that has 98% survival rate
Please cite a source here. Survival rate usually means IFR not CFR, and even the CDC's own number (the CDC is going to be incentivized to overstate risk) puts it at around a 99.4% general survival rate. Other estimates put it closer to 99.7% or even higher.
Good point, I hadn’t considered this. Also there was the factory QA issue. Possibly much like in aviation , multiple small factors here that need to be addressed and they’re using this as easy excuse to put pause.
This is possible, but I work in medical research, and this pause is pretty standard practice. When there is a potential problem, you pause, gather more data, come up with a mitigation plan (if needed) and submit all this to the ethics authority (usually IRB). Its rote standard practice. And i think much more likely that they are following standard practice than there are hidden issues that haven't otherwise been revealed publicly yet.
That said, this is not a usual situation at all, and I think it's absurd, not least because of lives potentially saved during this pause, but because of the carry on effects with vaccine hesitancy, etc.
Wrong. In a war you win by outsmarting other people. Maybe that's through democracy, maybe it's by moving faster, maybe it's by having better technology, maybe it's by having more technology.
This is a pandemic. A health crisis caused by a virus. In this situation you win by carefully understanding the nature of the virus and then determining what needs to happen in order to shut it down. Making rash decisions because it's "wartime" doesn't actually stop the virus. We can't blitz a virus. We have to take time to understand the consequences of our actions.
> coddle
Actually, we do have to coddle. If we squash people's concerns about the vaccine, then they just won't get it because they don't feel listened to. On the other hand, if we show people that we're taking their concerns seriously, they're more likely to go and take one of the other vaccines. Because the "unsafe" ones were pulled after all, so the ones left over have to be safe (not true, but it's going to work for a non-trivial number of people).
I don't think you're appreciating the magnitude of the error here. This kind of complacency, typical of the public health bureaucracy, has led to a large net increase in death.
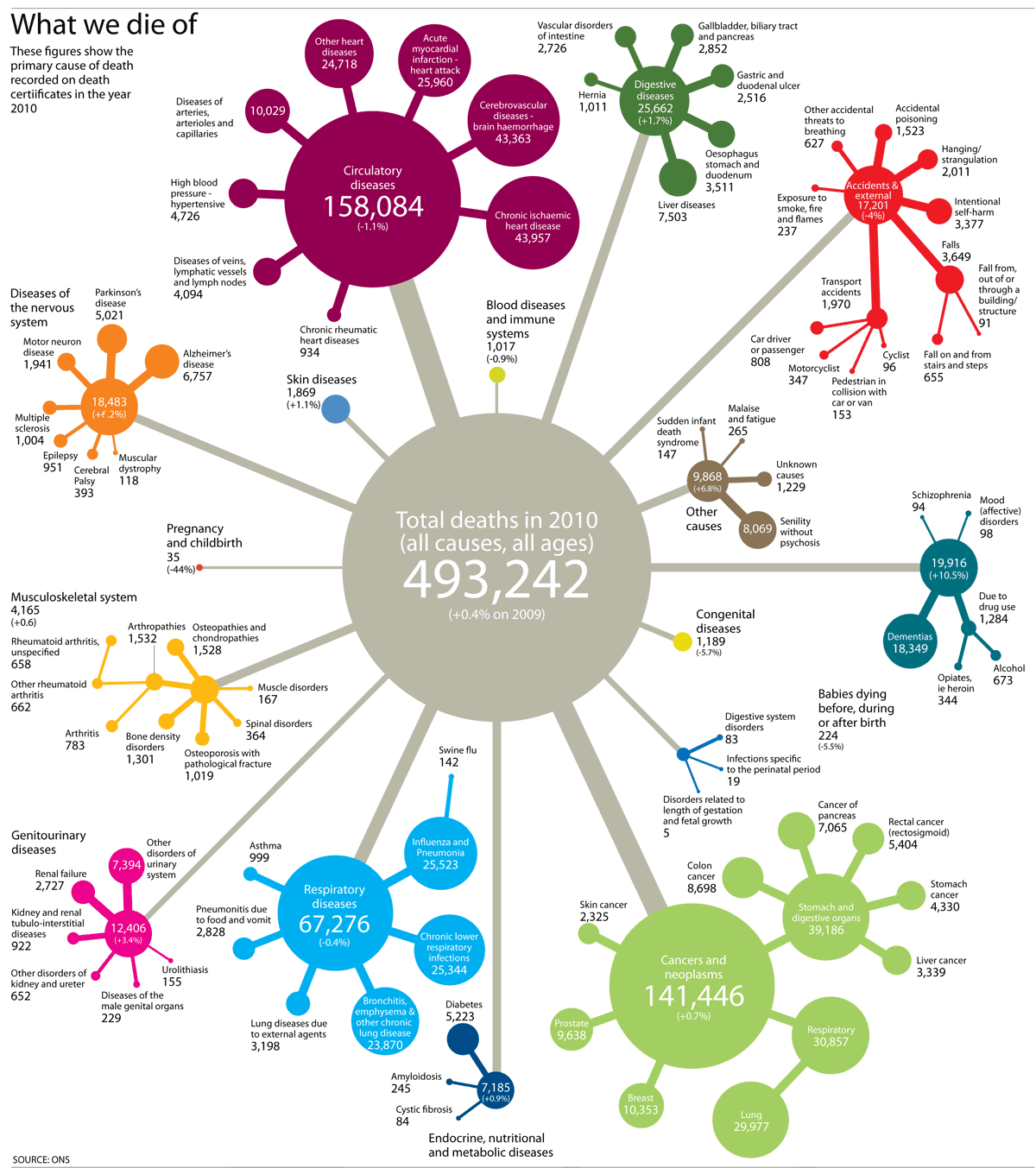{kind=link}