> Though insulin generally costs less than $10 per dose to produce, some versions of the drug have a list price above $200. This is in part because, in the US, a warped market has allowed three companies to dominate the insulin business.
> With California leading the way, a handful of states are considering trying to disrupt the market for essential medications, starting with insulin. The plan would be to manufacture and sell insulin themselves for a price that is roughly equivalent to the cost of production.
I feel like I'm missing something here. My understanding of why insulin is so expensive: laws are created and enforced by the government preventing people from competing in the space.
If you try to make your own insulin, and you take it to market with 3rd party analysis and certification of it being medical grade (and safe) insulin, you'll start seeing an escalation of the state against you. First angry letters from lawyers and eventually, if you continue head strong and ignore everyone telling you to stop, government officials (possibly with guns) will come and forcibly shut you down.
Is California just going to ignore these laws? How will the state not be liable for damages when individuals are?
I'm all in favor of revoking the legal structures that pick the winners in this market. It seems like there are plenty of people passionate in this space that would/could make insulin at near-cost if permitted to.
It's just that, by my understanding, it's the government that doesn't permit them to. It's weird that people in the government (at the state level) are stepping in to do what people in the government (at the federal, but possibly also the state level?) won't let people in the market do.
Edit: substituting “intellectual property laws” with “laws” as it seems there’s more to it than just IP.
A lot of formerly protected insulins, e.g. insulin glargine, are off patent now. The remaining moat for generics consists of FDA approval, delivery system patents, and manufacturing process patents/trade secrets. For a generic insulin to get FDA approval it needs bioequivalence which is a lot like running the original safety and effect studies over again, while dealing with spurious injunctions and the like from the company with the name brand. If you get to the finish line as a private company, you're going to price it where you can get some of the market but not get into a price war with the name brand.
California, on the other hand, is paying a lot of money to Novo Nordisk et al, and would benefit from reaching a low average price. They can afford to go through the approval process with all the important insulin analogs. And they won't go bankrupt in court before it pays off.
>. For a generic insulin to get FDA approval it needs bioequivalence which is a lot like running the original safety and effect studies over again
That is incorrect. A bioequivalence study is much simpler and cheaper than the original safety and efficacy studies.
You do not need to prove that safety and efficacy of the drug, only that you are delivering the equivalent of the originally studied drug at the same doses.
> I don't understand. My understanding of why insulin is so expensive: intellectual property laws are enforced by the government preventing businesses without that intellectual property to compete in the space.
That’s not an accurate understanding of intellectual property specifically. Insulin isn’t like a pill, where once you have a chemical formula you can make millions of them very cheaply. It’s a biologic, an artificial hormone. Even leaving aside the patents, it’s very expensive to get approval for a generic biologic (called a biosimilar). That’s why there are few manufacturers of synthetic human insulin, even though that’s out of patent.
Hi Rayiner, you are spot on with your analysis. My name is Eric, and my non-profit, Project Insulin, is tackling this problem head-on as well. We are developing a biosimilar insulin and will distribute it directly to patients at cost. The drug development process is still expensive but much cheaper because of the Biologics Act that was passed in 2020. When going through the FDA approval process, biosimilar insulin makers don't have to do phase 2 trials, and their phase 1 & phase 3 are focused on interchangeability with the reference product rather than proving that insulin is a way to lower high blood sugars.
Another obstacle, as you pointed out, is that there are few manufacturers who produce synthetic insulins. From what I've learned in my discussions with manufacturers is that many are transitioning their facilities to a focus on mRNA drug manufacturing. Therefore there is a limited set of manufacturers who don't make insulin but have the equipment/facilities for it (in the U.S.).
Hi Eric! I'm a T1D and so super interested in this space. Can you comment on whether it is the case that "modern" insulins (Lantus and Humalog/Novolog, in my case) are both covered by current patents, and also considerably better for patient outcomes (faster acting, more predictable -> lower A1c) than non-covered insulins? That is my understanding for why cheap, high quality insulins are not available, but I'd love to be informed if it is not the case! Thank you for your work in this area!
(not OP). some quick googling reveals lantus is no longer covered by patents. patents in the usa last 20y, and they filed the main patent for that drug in 1994.
it looks like they tried to patent some pen injection mechanism as a way to artificially extend the patent, but the patents were tossed out. I think that's a similar approach to how the Epi-pen people have maintained control, except their pursuit was successful (epinephrine isn't exactly a new chemical, nor is the process for manufacture).
still--manufacture of these drugs is long and expensive process, esp with fda approval. new entrants want to recoup their cost. the public is a great institution to develop generics because it can happily do so without a profit motive.
I think Humalog/Novalog patents expired a while back. These companies will probably focus on other newer drugs for profitability like Semaglutide which is useful for dealing T2D and obesity.
Another thing that needs to be investigated is how much the PBMs (Pharmacy Benefits Managers) prpfit from the spread of drug pricing. Are they marking these drugs up a lot? Do they need to be tightly regulated?
Hi as some of the others have already mentioned Lantus is off patent. My organization is focused on insulin glargine but there are generic versions of insulin lispro and aspart. Which is the generic/biosimilar version of humalog/novolog. We decided to stick with glargine first and transition to the other versions as we progress.
Hi Eric, my name is Francesco. In the last three years we industrialized a novel method for producing biosimilar insulin (in Italy). We are an international team and I really would like to contact you. Can you write to the email you find on my profile?
Hey Eric, somewhat tangential question -- why is it that seemingly all precursor manufacturing is done in China or India? Is it just a low-cost game or are regulations making it too expensive to do in the U.S. or something else?
This is a great question. Simply it is a lot cheaper to make drugs in China + India. The APIs cost less, and the workforce is cheaper. With regards to regulations I don't want to generalize but it has been well documented that it is hard for the FDA to regulate drugs being produced outside of the United States.
While I don't know the answer to this in-depth I can share some bullet points and of course it depends on what country you are talking about. On top of that it is important to note that there are insulin shortages in various countries.
- one payer healthcare systems
- non-convoluted distribution systems
- depending where cheaper workforce/cheaper to make the insulin
- less stringent regulatory processes
- stronger lobbying groups in the US
People dont want insulin (traditional insulin.) They want fancy insulin (modern insulin), because it is convenient. They want modern rapid and long acting insulin. They want pens. Maybe people want the inhalable powder. Those innovations exist outside the original insulin patent. They are also mixing other drugs with the insulin.
>Average retail prices of Novolin and Humulin (traditional short- and intermediate-acting insulins) have gone down, or held steady, while prices of modern rapid- and long-acting insulins continue to go up. On average, traditional insulins now cost less than half of what modern insulins cost.
There is a lot more going on that makes high end insulin expensive. A lot of conversation around insulin is people talking past each other because they are referring to different things that they think should be free, usually one of these additional features on top of the hormone itself.
I do agree with the statement that some of the language around the lack of insulin availability is misleading, but it's not just that it's more convenient. "Fancy" insulin allows one to better manage blood glucose levels. Poorly managed blood glucose strains various organs/systems in the body and over years and decades leads to various health complications, some resulting in death. (It's still a lot of work and stress -- modern insulin isn't an automatic improvement; but it does allow greater success in managing diabetes.)
(My comments here are in the context of type 1 diabetes. The (potential) positive health impact of modern insulin may be less pronounced for other diabetics.)
I dont mean to be dismissive or elitist. There is enough wrong with the medical system, that if somebody loses coverage and needs to see a doctor to get their prescription changed, that change alone becomes insurmountable, behavioral change not included.
My rub is that the conversation is dishonest. Saying "access to insulin is a right" and then changing the topic to modern delivery methods and such. Call a spade a spade, and have the direct honest conversation the first time. My pertubement goes beyond this topic into social justice/political correctness and just about anything. I may believe in the cause and the result, but be dismissive of how to get there by cheating and hacking peoples attention spans. It seems the only way to be an activist and get attention is to start with a lie, and now everybody is competing for the most inflammatory headline.
Everything you said is the conversation everybody should be having, instead of truncating it to "insulin is way too expensive."
I think a big problem is that short acting insulin, which was available 25 years ago, used to cost $9usd / 10 mL bottle now costs ~$80 with insurance (in california) or $200+ list price for an effectively equivalent short acting insulin. (numbers were from my insurance statements which include the cost for current prices, and from a family member who was on the pharma board at one of the large managed health facilities in california in the 90s.
To me, that cost inflation is purely artificial and not driven by any new tech relating to the insulin itself.
For T1 diabetics, the cost increases have been moving to insulin pumps which have infusion set costs in addition to the actual pump, and for continuous glucose sensors.
That's basically a 4.4x increase, after inflation to jump from short to rapid. Not saying its justified. Why pay $200 list for something that is less than $80.
Yeah, you can do some quite easy motte-and-bailey with it.
Everyone will agree that (cheap, out of patent) insulin should be available to all; it's literally lifesaving.
But then switching that to the (modern, convenient) insulin should be available to all is a bit of a slight of hand, especially when it is NOT a "you will die without this" but a "you will have more hassle taking medication to not die" scenario.
Obviously the costs involved in implementing these technologies should be part of the discussion, but I don't think it's unreasonable to want to make anything that eases management of diabetes way more affordable.
Which is what the conversation should be, and how it should be framed.
The press writing "life saving insulin" headlines takes away from the ability to discuss that: within the last decade or two, modern improvements made the process of managing diabetes significantly easier and else stressful. The drug companies gave everybody a taste of an easier life, and then jacked up the price, saying "pay us more or go back to the old way." At what level should the government step in and subsidize or control this quality of life improvement? At what level should its creators be rewarded?
I am old enough to remember when the entire world took traditional insulin. It wasn't pretty.
I would like to point out that these fancy insulins have been around since 1996. I do agree that there is cheaper insulin available, but as others mentioned there is a significant change in quality. But I agree with you that the conversation should be affordable high quality insulin.
Another piece of the insulin ad drug saga that I haven't seen many people discuss here is the distribution of drugs. The distribution from manufacturers to patients is incredibly inefficent with a variety of middle organizations increasing the cost associated with distributing the insulin and those costs are pushed down onto patients. Our website has a simplified graph showing the current model vs what we plan on doing: https://projectinsulin.org/why-insulin/
I assume when you say 1996, you mean Humalog/insulin lispro? That falls in the rapid category, but I feel like most of the conversation about people wanting cheap modern insulin is the long acting right? The primary quality of life improvement people seek is having to inject only once a day, plus extra if diet requires?
I was dating 20 years from glargine (invented 1994, approved 2000), which is technically still patent protected somehow, despite biosimilars being approved. It takes a while too for Doctors to switch over when new paradigms are delivered. The real metric should be when long acting overtook intermediate acting prescriptions.
yes apologies glargine was approved in 2000. And I agree it does take a while for doctors to switch. Something interesting that I have recently learned is that it may even be hard to find clinical trial participants because doctors will be hesitant to take patients who have good reactions to their current insulin off of that insulin to be a part of a clinical trial.
I will also say that Pharmacy Benefit Managers (PBMs) also have a lot of power when it comes to influencing doctors to begin prescribing new drugs.
> At what level should the government step in and subsidize or control this quality of life improvement? At what level should its creators be rewarded?
You assume that creators are rewarded.
In Sweden you get the insulin and pens for free (that is, you've paid for it with your taxes).
And it was invented there? When I say create I mean discovered not manufactured. The R&D.
And the answer/solution is somewhere in the realm of a public/private hybrid, where the government is funding short term expensive, long tail benefit research.
This is beside the point. You pay for insulin, but with taxes. In return, you don't have to deal with "do I eat or do I get insulin".
> When I say create I mean discovered not manufactured. The R&D.
The question remains: are the creators actually rewarded?
In the US most R&D now is performed by small companies, government entities, or with government money. Large companies buy this research cheap and profit from it immensely. There are cases when all new drugs that appear on the market are based on public government-funded research.
The amount of revenue that goes back into R&D decreased while revenues increased.
Novolin 70/30 ReliOn vial (10 mL; 100 iU/mL) has had a flat price since 2014. The Novolin 70/30 ReliOn FlexPen (3 mL; 100 iU/mL) pen has been the same price as the vial since mid 2018 when it came out.
The price of these drugs NEVER went up.
Framing it as only "more hassle" or "purely convenience" really downplays the difference in the quality of life improvement the last decade has brought everyone.
IANAL, but they may not be ignoring those laws; they may be planning to fight them. That cannot happen without standing, which may be easiest to obtain by trying to move forward with this plan.
I suspect they would be breaking federal laws, so I believe consideration of the State's 10th Amendment rights applies here. That would be wonderful and hope that this case brings that topic into the spotlight, because I see 90% of the federal government as being grossly unconstitutional on that basis alone.
Personally, I suspect the market leaders would not want to face the courts, because the exposure would be horrible PR that affects all of their product lines. Moreover, an aggressive and concerted effort to block this effort should be viewed as the anti-competitive behavior of a cartel, which is the status quo de facto that the State is effectively trying to disrupt.
I don't see such a challenge as anything but a lose-lose for those companies. Hopefully, they take the bait and do something stupid that leads to reform at the national level.
We already have precedent for a state outright saying "fuck copyright": Blackbeard's Law[0]. North Carolina copied a photographer's images and then passed a law saying the images were part of the public record and thus not copyrightable. The photographer sued to get the law repealed but SCOTUS decided that sovereign immunity meant there was no standing to overturn the law.
An interesting wrinkle is that Congress already foresaw this and passed a law decades ago waiving state sovereign immunity for patent and copyright claims. But then SCOTUS overturned the patent prong of this federal waiver on the grounds that Congress hadn't proven that states had a pattern of telling patent holders to go fuck themselves. And SCOTUS's reasoning for striking down the suit about Blackbeard's Law was that this also held true for the copyright prong of that law... despite being handed a brazen example of a state nullifying copyright law for their own gain on a silver platter.
What this technically means is that your state could, tomorrow, run their own pirate streaming site and not get sued for it[1]. The only way to stop it legally would be to sue end users, which would be difficult to do for a direct download service[2].
As for antitrust and cartels, since copyright and patents are legal, government-granted monopolies, most courts are very loathe to attack them even when they are used in ways that violate antitrust law. You can see this in FTC v. Qualcomm, where an appeals court smacked down an antitrust ruling for this reason. Compounding this is the fact that a very large contingent of judges have been slowly nullifying antitrust since the 1980s under the "consumer welfare" theory that every tech company is built to maximally exploit.
I could see California getting away with bloodying Eli Lily & Co's nose. But I would not count on this becoming a future model for evading (ab)use of the patent system. Remember, all the states are still part of a federal government that is very much in favor of the patent system as currently constituted, and there are still things they can do to block California.
[1] Assuming your state had not already waived sovereign immunity for copyright
[2] It's commonly believed that you can't sue for downloads, only uploads. This isn't quite true. At least one court has outright said that both are illegal but infringe on different exclusive rights. I don't remember which court.
> Is California just going to ignore these intellectual property laws? How will the state not be liable for damages when individuals are?
Insulin can be made without breaking patents. Unless you specifically require something branded as Lantus®, for example(which is in no small part due to publications funded by pharmaceutical companies themselves, but also some 'marketing' straight to doctors). There are other longer lasting insulin formulations that can be made.
There are hurdles if you take that route (as described in the article). Many are financial. One is regulatory (biosimilars).
> But pharma companies are savvy about finding ways to extend their monopolies, with insulin and other drugs, by making minor tweaks to the chemical compound and asking for a patent extension. In the case of insulin, the companies can also modify the delivery device to protect their market share. Each product is meant to be used with specific, company-designed injectors. Though the patents on the artificial insulin developed in the 1990s have started expiring, these companies continue to hold and extend monopolies on either their devices or other chemical compounds, making it harder for generic competitors to enter the market.
> Other federal regulations have added to the challenge. The FDA began to treat insulin as a biologic drug in 2020 — meaning it is made with living materials instead of combining chemicals like conventional pharmaceuticals — which comes with a different set of standards for generic versions, which are known as biosimilars, as well as manufacturing challenges given the precise conditions these products must be made in. Biosimilars can cost up to $250 million to produce and take up to eight years to bring to the market, versus a one-year investment of as little as $1 million for conventional generics. And unless the FDA recognizes a new generic insulin as interchangeable with the products already on the market, health insurers might not want to cover it and doctors may not be willing to prescribe it.
Seems like the barriers for a state entity are exactly the same as the barriers for private generic drug manufacturers, and the state could easily just stop erecting these barriers.
You know developing insulin doesn't require violating patents, right? And the price of insulin in the US is entirely an artifact of monopoly behavior by a small number of pharmaceutical companies?
The ability to mass produce insulin at negligible cost has been around for decades, they guy who discovered it made it patent free even.
Only in the US do companies get away with this kind of price gouging, and only because of monopolistic (or I get oligopolistic?) behavior and BS legal threats against anyone that might impact their profiteering off the work of others (paying off competitors not to compete, and BS patents on minor changes, with applications carefully scattered to maximize length of coverage).
The only reason it's taking someone the size of CA to actually do something, is because the Pharma companies buy out, pay off, or lawyer into oblivion anyone else. All strategies that normally work because the victims of the (to me) clearly illegal monopoly based actions aren't incurring costs if they stop, whereas the gouging and monopoly tactics cost CA huge amounts annually. The only thing Pharma could do to make it worth CA not doing this would be to stop price gouging, which is of course the only reason CA is doing this.
That price gouging is illegal if it's some dude hoarding toilet paper, but not when it's insulin being sold by multi-billion dollar corporations remains absurd. That people come to defend the "IP rights" of these organizations and their BS patents is a really American phenomenon.
The whole point of this is that insulin is more expensive in the US than elsewhere. So maybe it isn't "cheap", the point is the price is being inflated due to many factors, including through monopoly tactics such as paying off competitors to not compete.
Traditional insulin is cheap in the US. The price has not changed in a decade. Nobody wants it, it is a product of last resort.
Modern insulin is protected by moats, two of which are intellectual property and regulatory approval. Modern insulin being cheaper in other countries is because they are not following the same trade and approval laws. The way to match abroad prices would be to change protections and approvals, the latter of which is and has been happening over the last five years.
You are missing the point. Every kind of insulin is more expensive in the US than _every_ other country. It's not just old stuff is "cheap", new stuff is expensive. It's old stuff is more expensive in the US, new stuff is more expensive in the US.
Average prices per "standard unit"
* Rapid acting: $120 (US) vs $13.50 (JP)
* Rapid-int (?) acting: $107(US) vs. $13 (JP)
* Short-acting: $87 (US) vs $19 (FR)
* Short-int acting: $95 (US) vs $13 (JP)
* Intermediate acting: $73 (US) vs $13 (JP)
* Long acting: $88 (US) vs $15 (JP)
Novolin/ReliOn is nowhere near that expensive. I skimmed it, but report you are citing appears to be averaging the price of insulin types. So if there is a cheap rapid and an expensive rapid, it ignores that somebody can buy the cheap one. That averaging distorts the price of available traditional insulin dramatically.
It is more expensive in the United States because the US is subsidizing the earnings requirements the companies who make the drug require to develop new variants. At a high level, everybody pays insurance, it gets funneled into high drug prices, high drug prices pay shareholders and fund R&D. It's capitalisms version of socialized drug creation, and the rest of the world benefits from the US overpaying.
Even the modern rapid acting insulin that doctors are prescribing (Humalog, Basaglar, etc.) can be very expensive.
CVS filled a month supply for me after my insurance number had changed and when I went to pick it up they kindly asked for $1300 before I gave them the new insurance info.
Rapid (minutes) being modern insulin. Short acting (takes 30 minutes) being traditional insulin. Rapid for the most part being an additional technology and convenience over short acting traditional.
Nothing weird about that, it's the essence of federalism. The resilience of the American system of government is attributable in large part to federalism, the marketplace of ideas from the states competing with each other.
There is no patent on insulin, just regulatory capture on which proprietary analogs are approved for medical use. In 2020 the FDA changed the regulatory status of insulin, signaling that it's not going to let that regulatory capture continue. But if it does, there will be a lawsuit, it will go to the Supreme Court, and the pharma companies' arguments will probably get thrown out.
Insulin is off patent. There are new versions that offer a variety of benefits under patent, but just generic insulin can be made by anyone who passes the governments regulations. Walmart is known for offering generic insulin at lower prices.
Insulin pricing isn't entirely IP issue; it's been out of protection and available as a generic for many decades now.
The issue is that while insulin is actually quite cheap to make once you get started, the startup-costs associated with getting to that point are quite hefty: lab real estate, equipment to make and purify, FDA fees, etc.
Newer versions of insulin are "better" than generic insulin: easier to take, fewer side effects, etc. The major insulin producers have been slowly doling out minor improvements over time, about every decade or so, to maintain IP protection on these newer modern versions of insulin, and the high prices associated with these newer versions. They've also been paying off several generics manufacturers to delay them from manufacturing generic versions of these modern versions as the patents expire.
> Newer versions of insulin are "better" than generic insulin: easier to take, fewer side effects, etc.
Even that is debatable. At least Sanofi has been known to fund some rosy articles about their Lantus® product. When the EU looked into it (for similar initiatives) they were not able to find the large 'performance' gap that was suggested between that insulin and alternatives.
As far as I know, the major difference between insulin types is not their performance, but how long they take to act, when they peak and for how long they have an effect. Some types of insulin, like glargine (as in Lantus®) can be more convenient due to their long-acting response that lasts for an entire day.
I suppose off-patent insulin could be produced with some degree of inconvenience to the consumer because they might have to take more doses per day, but they should work nonetheless.
Long acting insulin is exactly what this entire debate has always been about. Generic standard insulin has been cheap at walmart forever. They even sell cheap rapid acting ReliOn.
People want long acting insulin cheap. (short-, intermediate-, rapid-, and long-acting, ultra-long-acting (42h) insulin are the main categories.) Long acting insulin was the product that had a price jump at the end of 2017.
I am pretty sympathetic to the non long acting stuff not being good enough. Expecting people to monitor hour after hour, and only calling it an inconvenience really downplays how tedious it is to stay alive.
T1D patients use both types if they are self-injecting. The long acting covers your basal rate (baseline) and the fast acting covers carbs you eat.
Or if you have a pod or pump then you can use only the rapid acting and the software will drip it slowly to cover your basal need over the 24h.
Trying to use just the fast acting with self-injections doesn’t work because you go high overnight while you’re sleeping, and even during the day you would have to be injecting every 3 hours to keep up. (E.g. when your pump controller dies on vacation and all you have on hand is rapid-acting)
Which would be covered by traditional mixed, short and intermediate insulin, right? The price of Novolin 70/30 (mixed), Novolin R (rapid) and Novolin N (intermediate) insulin have remained flat since 2014. (Short acting and Rapid are two different things, the former being the old kind of insulin that takes 30 minutes, the latter being modern tech that takes minutes.)
It's when you want something better, that lasts longer than Novolin N that price starts to go up. (Novolin N is typically injected underneath the skin (subcutaneously) once or twice per day.)
Obviously, if you have insurance, I would expect you to be being prescribed something better, because that's how the world works. Then you can jump from traditional insulin to rapid and long lasting, and pens.
> They've also been paying off several generics manufacturers to delay them from manufacturing generic versions of these modern versions as the patents expire.
Isn't that already illegal (price fixing/collusion)? How are they structuring the deals to avoid prosecution?
The inventor of insulin sold the patent in 1923 to the University of Toronto for one dollar so that nobody could take advantage of people in the way that's currently being done.
This is 100 year old technology. It has nothing to do with development cost.
There’s not a single word in that entire article that calls out that modern insulin products are not the same animal-derived insulin that was isolated 100 years ago.
> I feel like I'm missing something here. My understanding of why insulin is so expensive: laws are created and enforced by the government preventing people from competing in the space
The article doesn't do a good job of explaining that "insulin" isn't a single drug, or at least how they describe it.
Generic insulin is cheap. You can get it for $25/vial from your local Walmart. With production costs, regulation compliance, storage, transport, and paying pharmacists, they're not making much profit on that.
Patented insulin analogs are not cheap. They have different characteristics for duration and onset time that make them easier to dose, but the patent means that you can't produce and sell it unless you own the patent or have licensed it. Drug companies who own these patents set their prices according to what they can get insurers to pay, not according to what they expect people to pay out of pocket.
One of the weird quirks of the US medical system is that drug companies often have alternate prices for people without insurance. Remember, the high prices aren't designed for you to pay, the high prices are designed to extract as much money as possible from your insurance company.
You can see this in action on drug company websites. Lilly has a program that will cap your payments at $35 for even their expensive insulin analogs: https://www.insulinaffordability.com/ You have to renew every 12 months and hope they're still doing it, but they generally keep these programs around because it dampens the outrage about the high prices.
If it was about intellectual property then it would not be tens of times cheaper in the EU and other countries. Insulin is not something new and advanced that needs special protection
What you’re missing here, just like how everything runs in California (and perhaps in most places), the government won’t be in the business of manufacturing insulin. They will choose a winner to be the subcontractor to produce the product. That firm will meet a price point for the duration of the contract and then renegotiate. Or go into the market like the other players.
California will make insulins already off patent. Ones where lower cost versions are already available. It would be far smarter to just subsidize existing versions.
But it doesnt solve the problem that the latest cutting edge patented insulins cant be copied by the government.
Not knowing anything about the specifics of California, but bad law here seems to follow a rough process:
1. Centralise power in a regulatory body that will raise costs every time something goes wrong.
2. The barrier to getting things done rises until there is a crisis.
3. The barrier is so high only someone behaving like a financial illiterate would enter the market, so legislators task government with entering the market or underwriting someone who can.
So I'd assume that legal ability that was ever the problem. Usually it is regulatory requirements implying a minimum size of the actor needed to take on the risk. I see a few comments that this time around the technical term implementing this for insulin is "bioequivalence" but the broader pattern applies in a few markets and should be called out.
This is great news. Honestly, I hope to see more nationalization of widely used services (or whatever the equivalent word for nationalization is at state or municipal levels.)
Municipal broadband, power, roads, schools, post, housing, and healthcare? It's long overdue, and with an appropriate amount of funding has been shown to be effective at controlling costs and delivering moderately good quality in most cases.
A lot of things get so warped by profit motive. And there are places I want a profit motive, but insulin (and healthcare generally) isn't one.
Honestly though some industry's products/services verifiably don't improve end user/customer experiences from maximizing profits. It's hard not to see it at this point
It makes sense that to improve end user experience you need competition. Works great in restaurants. Anywhere with network effects (utilities) or legal barriers to entry (healthcare) doesn't tend to compete away poor results.
You say that as if healthcare isn't extremely regulated already and as if the regulation weren't a big factor in allowing these companies to monopolize the production of insulin. (Or, my favorite example back when I needed the stuff, colchisine.)
In the case of municipal broadband it mostly comes from communities that suffer form poor/no investment from the big players and is the only recourse for decent internet. It usually is faster and cheaper than existing solutions. There's clearly market failure here and players abusing their local monopolies to refrain from investing / provide decent service.
The state of telco in the US is pretty shocking, even in places like NY state.
> Municipal broadband, power, roads, schools, post, housing, and healthcare? It's long overdue, and with an appropriate amount of funding has been shown to be effective at controlling costs and delivering moderately good quality in most cases.
Where? The US has among the highest percentage of kids going to government owned and operated schools. We have plenty of government housing as well (projects). Nearly all of our roads and transit systems are publicly owned and operated too.
Almost uniformly, those government operated systems aren’t very good—in America. And it doesn’t have to do with “funding.” If you compare with Europe, we spend more money per student, per transit rider, and per public housing resident, etc.
Its easy to point at what doesn't work well, there's tons and tons of things that work great that nobody talks about.
Municipal broadband: the best broadband in the entire United States is provided by the municipality of Chattanooga. [1]
Post: The USPS is the most trusted brand in the United States, above FedEx and UPS. [2]
Transit: The New York City Subway is the 3rd largest metro rail system on earth after London and Guangzhou. Ok fine, it's expensive to build - but it moved 1,300,000,000 people in 2021.
> Transit: The New York City Subway is the 3rd largest metro rail system on earth after London and Guangzhou
It’s also the worst large metro system, by timeliness and reliability, in the world, despite being very well funded.
People in the rest of the country aren’t exactly unaware of New York. But its transit, housing, and public school systems are a poster child for how government-run services are terrible, even when well funded. There’s a reason why New York has suffered net domestic outmigration for many years.
Look, if Stockholm was in America the American public would have a very different idea of what government-run services could be like. But we don’t have Swedes running our government services, we have Americans. It is what it is.
> It’s also the worst large metro system, by timeliness and reliability, in the world, despite being very well funded.
You forgot to mention cleanliness, comfort, and safety, where it also is just atrocious compared to other metro systems outside US.
Praising NYC subway for being really big sounds to me similar to Soviet Union boasting how many tons of steel it produced. It sure did, but its citizens would have preferred instead to get something other than 1000 additional tanks.
> Municipal broadband: the best broadband in the entire United States is provided by the municipality of Chattanooga.
You can even get 25G from EPB now, though the 10G is good enough for me, frankly. That being said, there's several locations in the US where 10G residential fiber is broadly available; frequently either municipal or co-op (e.g. Utopia Fiber in Utah), though I believe EPB was first in 2015.
American schooling sucks because it's beholden to political objectives contrary to the interests of educating children. Look at the manufactured controversy over "intelligent design" a few decades back, or the current controversies over transgender bathroom access, or Florida's censorship of material in school libraries[0].
Municipal broadband and the post works well because the US is good at building infrastructure. But at the same time, our government is also beholden to interests that want to kill that infrastructure so they can sell costlier and worse equivalents. States passed a bunch of laws to ban local government from running ISPs and Congress has been putting stupid funding mandates on the USPS's pension schemes that make a profitable public venture unprofitable.
Transit is a bad example because America is famously addicted to cars and allergic to any transit system that isn't a road. The NYC Subway could not be built today under the current political climate. Hell, it wasn't even built by the city or state government; it was stolen from the people who built the system through overregulation. Nationally, we have Amtrak[1], which was created by bailing out failing freight companies. With some high-speed upgrades it could be great, but the system is still beholden to those same freight companies' infrastructure[2].
The underlying problem is that America does not want to build working government programs. It is run by people who deliberately take funding in order to burn it so they can complain about how much better "privately-run" monopolized systems are.
[0] There are probably examples that right-wingers would point out as well - maybe check Reason or CATO for them, because I forgot.
[1] US citizen: Japan has high-speed bullet trains! We should build a Shinkansen!
US: We have a Shinkansen at home.
Shinkansen at home:
[2] Which, BTW, is actually supposed to give Amtrak priority over the rails. Like it says it in the actual law. Nobody cares.
None of this has anything to do with why school sucks. Schooling sucks because it's erratically funded.
Wealthy families arrange to live in suburbs designed explicitly to cordon their children off from there less wealthy peers, each time setting up a vicious cycle where homes in those school districts derive much of their value from school funding, creating an incentive for an ever-increasing levy for de-facto private schools.
Meanwhile, big city school districts are relatively well funded (teachers in the largest cities have surprisingly strong compensation) but poor management. Not everything that Republicans say about teacher unions is wrong, and there is an extent to which management of city public schools is set up to allow schools with high parental engagement (= greater parent wealth) to succeed while others fail.
Simultaneously, if you look at school districts in poorer exurbs or, worst of all, downstate/upstate rural districts, teachers really are making the wages that TV shows make jokes about, supplies are scarce and enrichment classes (in some places) nonexistent.
These are structural problems, not culture-war-of-the-moment problems.
I'm not high-horsing any of this; my kids went to school in Oak Park, IL; I believe every full-time teacher at OPRF makes a six figure salary. Oak Park is essentially a pair of extremely well funded school districts (K-8 and high school) with a fire and police department tacked onto the side.
I agree with what you wrote and would add that a lot of times we’re only talking about schools because that’s how we fund a lot of social services in the United States.
My wife is a public school teacher here in DC. You can always find examples of the popular culture war hobby-horses, but most of the time when a student isn’t doing well it comes down to money. It hurts hearing about a kid who’s trying but falling behind since they haven’t slept more than two consecutive nights in the same place since a parent lost a job, or the top kid in the class cancels their SAT test because they need to watch a younger sibling because their mother can’t afford to miss work. When it comes to stats, that shows up for the school even if the student can’t.
There are many causes of lackluster public education, and funding is definitely one of them. Another huge one is the ability of parents who have the time and resources to divert their children (likely already at a huge advantage) to private and charter schools, thereby skewing the public school below the median in a vicious circle. I’ve seen this exact dynamic play out in many of the cities I have lived. It’s also why newer suburbs (avoiding legacy costs and filled with upwardly mobile, resourced families) have excellent public schools.
It's difficult to overstate just how huge selection bias can get in the education space. I went to a high school in the Bay Area, one of a handful in my city. (1) Houses in our attendance area were ~$500,000+x more expensive than ones right across the street in another attendance area, because our school was "better". Why was it better? Because the parents paying an extra half million dollars to get their kid into a better school were going to make sure their kid did better, come hell or high water. So there were lots and lots and lots of after-school tutoring centers, where students would get taught the highschool material in advance, so that they would already know it forward and back when they were tested on it. Which makes the school test well, and thus look better than the other schools in the area, raising housing prices. x += $100,000; GOTO (1).
The actual quality of the education was substandard, but there is something to be said for being embedded in an environment where academic failure was simply not considered an option.
The increase mentioned in your article was in the last 4 years? Seems a bit late for the testing outcomes in your original link. Pretty terrible example. Also, that area is a perfect example of where parents with the means move their kids (and their attention) to charter/private operations, exacerbating the problem.
If you study the insulin pricing issue carefully, you will find that largely the problem is government, not the market.
The profit motive coupled with competition works very well to keep prices low.
You need only realize the following; European firms stand at the ready to supply insulin at well below US prices today, but are prevented from doing so by the FDA. And they can do so and still turn a profit.
> has been shown to be effective at controlling costs
That has never happened. What does happen is the cost is borne by the taxpayer rather than the user of the service.
The "warping" of the profit motive in the insulin case is entirely caused by government interference and regulation (by making it nearly impossible for competitors to spin up and make insulin).
Not really. The internet is an example of what happens when you suck margin out of high margin businesses like content creators. India is an example for pharmaceuticals.
If the state takes a commodity and sells it on a cost plus or cost basis, it’s going to kill investment in the spaces and collapse the margin.
At this point, we’re killing people and bankrupting states and employees with out of control costs. Making an example out of insulin would fix that and constrain some of the players in the market.
Who do you think is paying now? States are spending billions on it through Medicaid cost share.
A state like California with a contract manufacturer would probably break even on the insulin and save billions for reduced complications. Poor people with diabetes are frequent fliers for ER admissions. The cost of one ER visit is probably close to annual insulin cost.
Why make the jump directly to central economic planning? I mean what it sounds like you're saying is communism is when the government buys things? So not a big fan of like, roads?
Are you arguing in favor for no government regulations whatsoever? Are you arguing for cartel state?
Earlier you said the warping of insulin cost is caused by government regulation. It sounds like you're not differentiating between central economic planning, the government "running things," and regulation.
I'm confused by this because it seems a purposefully black and white take.
I don't use "central economic planning" unless I'm talking about a State that has implemented, well, central economic planning. It doesn't make sense to me to point to a country with nationalized transit and nothing else nationalized, and say "they do centralized economic planning." How are you differentiating between these two kinds of states? Because otherwise I don't know how to communicate the difference between the Soviet Union and, idk, Spain or whatever.
I'm also confused by the conflation of that with "the government running things." The government runs the military, is that central economic planning? The government "runs" elections, is that central economic planning? The government sends soldiers to break strikes, is that central economic planning? FEMA sends food and medicine to hurricane disaster zones, is that central economic planning? Is a firetruck central economic planning? Where does it end lol?
Finally the most confusing thing to me is where you stand on any form of government regulation. Happily it sounds like you aren't Full Libertarian and think Amazon should be building our roads, but when you say "the government running things" is the same as the government regulating things like how medicines can be produced and tested, I get totally confused. So a law that says "no murcury in medicine" is the same as... Central economic planning? It's equivalent to a nationalized healthcare system? That's weird because people have been arguing for the usa to socialize its healthcare system for decades but apparently it's already socialized, cause it has regulation?
I only am pinning you down so hard on this because I completely disagree that whatever people mean by "free market" is a means to greater material conditions for people, but I genuinely can't even figure out if that's what you're arguing for, I'm just working off my understanding of your world view from the other thread where you dropped a simple "this would be better if the free market did it."
There are far better ways of doing that. For example, government agriculture, because feeding people prevents them from dying, is still a bad idea, because every time the government took over agriculture, people died of starvation. Free markets produce a food surplus.
Where is there a free market for agriculture? The usa subsidizes farmers to control volume and prevent surplus overrun. Prices of food are thus artificially high.
In this case the regulation is certainly being pushed by the pharma companies themselves as they wish to use regulation as a means of eliminating their competition so they can charge monopoly prices. So less regulation is not going to help, rather, the political influence of the corporations is the problem. Doing an end run around the whole mess by simply producing your own insulin will rapidly cause collapse in prices as those companies will suddenly have competition, even if from a state run agency. It's happened many times before.
There are many cases where the government can produce things at cost and bankrupt for profit companies. It's not always effective but the situation is quite dire at this point
I listened to the Vox The Weeds podcast interviewing the same author and was frustrated that his many explanations seemed disconnected. Since old insulin patents have expired, is it that you are allowed to buy generic insulin but there are no manufacturers, or that you not allowed to buy generic insulin because recent advancements are so good that doctors won’t prescribe the old stuff anymore? And no one will make generic insulin because the brand-name companies will undercut them and there are so many kinds you need to make, but basically a $100 million donation to the world by California will fix all that?
You are allowed to buy generic/affordable "older" varieties of insulin. It can be got at Walmart for $25 per vial. It is a "regular insulin" as opposed to the more modern insulin analogs; a functional but inferior technology that requires a very restrictive and rigid diet, as opposed to modern combinations of fast and slow acting analogs that allow for something closer to a "normal", albeit carb-cautious diet. It will, to quote my endocrinologist, "keep you alive". It is not part of a modern regimen for a Type 1 Diabetic.
My understanding is that it is manufactured by Novo Nordisk, the makers of more modern, name-brand insulins, as well (they make the fast-acting insulin aspart called Novolog that I take as part of my own regimen).
Yeah, I don't mean to decry their effectiveness, only what they demand of the user in order to render that effectiveness. They were the gold standard up until relatively recently, and saved a lot of lives.
The modern programs of a combination of fast/slow analogs are more flexible and adaptable. The demand on the user is still pretty high, but it's a bit closer to baseline.
EDIT: and I guess I should say, I've got plenty of bias from my own relatively narrow experience. I'm sure there are different regimens and different opinions amongst various doctors
> Since old insulin patents have expired, is it that you are allowed to buy generic insulin but there are no manufacturers, or that you not allowed to buy generic insulin because recent advancements are so good that doctors won’t prescribe the old stuff anymore?
Walmart sells human insulin (the previous gen stuff) for $25/vial. It’s manufactured by Novo Nordisk. It’s what was regularly prescribed in the 1990s. It has downsides, such as requiring a strict eating schedule: https://diabetesstrong.com/walmart-insulin/
Most doctors today prescribe human analog insulin. They do this because it is better at controlling blood sugar without requiring strict eating schedules.
In my experience at least, yes, there are many types. However, a few types are remarkably common and overpriced. In terms of a tech metaphor, it’d be like making Ubuntu and Windows 10 available for all after having them severely restricted. And yes, I know Ubuntu is free, but the point was to demonstrate how common the most popular insulins are.
Are the popular types of insulin still under patent, and if so, how is California’s initiative a solution? Are they hoping to license the necessary patents?
The insulin that California would be getting from Civica Rx, at least, would be analog insulins. They are partnering together until California can make its own insulin. The biosimilars made by Mylan (Semglee) and Eli Lily (Basaglar) are both analog biosimilars, specifically biosimilar insulin glargine.
> States have become more ambitious in their policies for tackling the insulin affordability crisis because the scale of the problem continues to grow and the federal government seems capable of taking only limited action to address it.
As if the federal government isn't the one causing the shortage in the first place.
> When a company develops a new drug, it gets a period of exclusivity, 10 years or more, in which it is the only one able to make or sell that drug. But after that exclusivity period has passed, other companies can make a carbon copy and sell it at a lower price. Studies find that once several generic competitors come on the market, prices drop significantly.
# 2 big pharma has hacked regulations for prescription drugs, medical devices and generic replacement to prevent losing federal government granted monopolies.
> But pharma companies are savvy about finding ways to extend their monopolies, with insulin and other drugs, by making minor tweaks to the chemical compound and asking for a patent extension. In the case of insulin, the companies can also modify the delivery device to protect their market share. Each product is meant to be used with specific, company-designed injectors.
Regulations often have the effect of protecting entrenched corporate interests.
Government regulation hurting competition, and hurting the free market by "protecting corporate interests too much" is precisely what people are often complaining about.
Supporting the free market would instead be when you allow competition, and do not protect the entrenched corporations too much.
Copyright and IP laws are probably the quintessential example of government harming the free market by preventing competitors from competing.
"All these safety regulations slow down the free market! Anyone should be able to make and sell insulin! If it's poisonous, people just won't buy that!"
For sure, but also I don't want "Joe's Discount Basement Insulin" to be on the market. I do think we should allow imports of medicines from some places in the world as long as they meet a verifiable safety standard.
We could also just nationalize the drug industry. Public funds pay for research already don't they? Why even let corporations in on this, just do it all ourselves and let the sociopaths go exploit adtech or some shit that's less likely to get people killed.
Insulin is typically delivered by a pump device that monitors patients blood sugar levels and doses accordingly. The pump is a medical device too that is manufactured by the drugco. It only accepts insulin vials from drugco.
It's like the inkjet printers that refuse to use ink from other vendors.
My insulin pumps take any insulin I fill it with. I’ve never heard of pumps that only take a specifically manufactured vial. Which one are you referring to?
Also, the pump manufacturer is not the same company as the insulin manufacturer.
I think what the GP was trying to say is they could easily solve this problem however letting it happen and blabbering about fixing the issue is easier and more profitable than actually doing anything.
> The state is taking a two-phase approach. In the short term, California has put out a request for proposals from existing enterprises that could produce generic insulin for the state as a subcontractor in the next few years in order to try to deliver relief as soon as possible.
[...]
> But in the long term, the plan is for a government factory operated by government workers producing government-owned medication. The state would have its own public production facilities, staffed by civil workers, which would sell generic insulin for the same cost needed to produce it, plus perhaps a small percentage to cover auxiliary costs for the program.
> The $100 million in funding is split evenly between the short and long term. But that long-term vision will take time. Even if the state were to retrofit an existing factory for insulin production, that construction work could take years, as would hiring a workforce to oversee it. Once production is up and running, California would need to hit more targets — most importantly producing a product that the FDA says is interchangeable with existing insulin medications.
That second phase is certainly ambitious. Putting it out for bid would be the more normal government process. It will be interesting to see what happens.
Newsom structures things like this a lot, and the more ambitious part almost never happens. I think this is mostly about running for president and creating a talking point, call me cynical but I don't think anyone expects Ca to directly run drug manufacturing.
Don't believe in Gavin Newsom's new bullshit.
Last I heard about this, a Vial of generic insulin was going to be $35.
Walmart sells the same insulin (regular or suspended varieties) for $25
It is just a publicity ploy.
Even at $25/vial, Walmart insulin has a very nice mark-up. Why buy it from state of CA for a more expensive price tag?
To boot all of this, if you do not have health insurance, Walmart sells the insulin to you without prescription. CA? Not so much.
I am sick and tired of this quasi-populist sounding stories from California nad other liberal inundated locations.
I thought that insulin was the rapid one and not the long lasting one. I think a lot of people had put themselves into diabetic shock by using that one instead of the one they needed...because it was cheap.
This is the more modern insulin analog, insulin aspart (sold branded as "Novolog"). It is fast acting, and has a different treatment approach than traditional human "regular" insulin. Using it incorrectly or recklessly definitely risks a hypoglycemic incident, which can be fatal. Selling this under the ReliOn brand is new, and it is relatively affordable compared to the sticker prices for the branded versions (upwards of $300 for a box of 5 pens, vs. the $73 walmart is offering)
Walmart also sells, and has for a while, "regular" human insulin under their "ReliOn" brand, which is $25/vial. This is an older style of insulin, less flexible and reactive, and requires a more restrictive lifestyle to make it work . Not following this restrictive diet schedule and rules can put you at risk of a hypoglycemic incident, which can be fatal.
There are other kinds of insulin analogs, including a "slow acting" variety called insulin glargine (sold under the brand names Basaglar, Lantus, etc). It serves to smooth the overall curve of blood sugar on a given day. My own treatment regime includes both insulin aspart and insulin glargine. I do not believe Walmart sells any insulin glargine (yet?)
For what it's worth, as an additional piece of information, a Continuous Glucose Monitor (CGM) is another modern tool in the treatment arsenal. They are also incredibly expensive, especially without insurance, but have saved my life several times when I made mistakes or just had bad luck with a dose of insulin aspart, and went very low. Being able to see myself starting to go low, rather than simply reacting when it is too late and I am already affected, is a significant aid.
As someone with little actual knowledge of different insulin, I've been told that the cheaper one that Walmart sells is significantly harder to manager and you tend to end up going through lots of spikes & dips with it, which while enough to still live for some is pretty debilitating.
Hopefully California is planning on doing a different style of insulin that better manages that?
That's incorrect. For a long time, Walmart has sold an older, human insulin. This is a relatively new product which is an analog insulin. It's the same NovoLog that's widely prescribed just with the ReliOn brand stuck on it.
Unfortunately, this is true, and a lot of people struggle to manage their diabetes after switching to the Walmart brand. The stories I have heard generally occur to young adults who have to transition out of their parents' insurance plans.
This article is from 2019 and is out of date. It's saying that Walmart only sells human insulin which isn't true any more. ReliOn NovoLog is a modern, analog insulin and is exactly the same as "regular" NovoLog:
Walmart needs to either earn a profit or use the item as a loss leader to earn a profit elsewhere. A government can provide services without expecting them to be profitable. (See: roads, licensing, schools, transit, etc.)
There's no reason California couldn't say, "If you need insulin, and you live in California, it's available for free." Assuming that's what the taxpayers want.
> A government can provide services without expecting them to be profitable
Governments are just collections of people organized by incentives, just like corporations.
In corporations, the profit incentive pushes the organization to minimize the cost of production. At the same time, competition puts a ceiling in prices. Poorly organized, staffed and managed businesses go bankrupt.
In a government, there is no incentive to minimize costs. Next years budget is contingent on isi h all of this years. Leadership positions are politically appointed, not based on competency. Employees are not rewarded with huge bonuses or promotions for competing projects on time or ahead of schedule. Budgets can just be sink holes, as long as they are politically expedient and have the proper messaging. Better ideas are routinely stifled by political agendas, and investment is singular; one department gets all the funding and there is no competition.
Look at Venezuela as an example. When the government nationalized the oil industry, it completely fell apart. Production dropped off hugely.
I clicked on the Vox link, hoping to see an update. There wasn't one, although I'm guessing that the 2022 announcement was about the budget being approved and now in 2023, they just started writing an RFP.
About 3 in 4 enrollees in ACA plans that use insulin pay $35/month or less out of pocket. For people with private insurance, 4 in 5 pay $35/month or less.
The biggest problem seems to be too many plans, too many choices, and too many ways to fall through the cracks.
Yeah, it's important to note that all the money the insurance company pays for medicine is still coming from you and other policy holders, it's just in the form of a predictable monthly policy plan instead of a possibly very large unexpected bill. If the drugs were cheaper, you could get a cheaper insurance plan that offered the same quality of coverage. So extremely high insulin prices hurt you even if you personally don't take insulin.
I think a part of the trick here too is that this report does not appear to discriminate between Type 1 (where insulin is required, and the amount required varies significantly and often increases with age) and Type 2 (where insulin, if it is required at all, is often required less).
Folks in the Type 1 boat are in a much rougher place without insurance than the far larger, and growing, population of Type 2s. And I imagine, skew any reporting that does not make the discrimination between the two.
(This all intended as a supplement to your very good point)
Also, no one is paying sticker price. When I was uninsured I often payed less out of pocket costs for care and medicine because so many automatic discounts kicked in.
Drug costs in general are jacked up in the US. Insurance will "negotiate" but ends up paying anyway. No insurance, you pay the full price.
Insulin is cheap. My brother gets his from the Brazilian government, no charge and no proof of income(it is a life-saving medication and you already pay your taxes). If you want more "convenience" (receive at home, not wait in line, etc), you can go to a pharmacy and pay. Costs maybe $20 for a month's supply of brand name long acting insulin (less if you are low income, even less if you have some forms of private insurance).
The Brazilian government also highly incentivizes generics vs brand names, doctors will often prescribe by the active ingredient unless there's a very specific reason to go to a particular brand. It has threatened to break patents (and done so on occasion) of companies that overcharge for essential medication (https://www.reuters.com/article/us-merck-brazil/brazil-bypas...)
There is absolutely no way insulin costs should be as high as they are. Walmart survives with a 3% profit margin but somehow we allow pharmaceutical companies to charge about whatever they want. It's not 'high tech' anymore, despite minor improvements by Lilly and friends to keep the patents alive.
Related: US health care costs (global is following) are also higher than they should because of the food industry. They will push their sugar heavy processed crap worldwide, but in the US they use high fructose corn syrup. For decades fructose was erroneously pushed to diabetics because fructose doesn't raise insulin levels. What it does do it cause metabolic syndrome, ultimately leading to obesity, type-2 diabetes, and there are links to cancer and even a growing number of publication linking to Alzheimer's and dementia in general. 88% of Americans have some sort of metabolic dysfunction(https://www.ksl.com/article/50332891/88-of-americans-are-met...).
We tend to shame people and say that they are pre-diabetic, obese or what have you because they are lazy and over eat. That's untrue. You can't outrun a bad diet. People will try to "eat healthy" and eat a bowl of cereal because companies say it's good for you. It is not. They will cut fat (and end up eating more carbs) because they have been told (by the food industry) that fat is bad. It is not, sugar and highly processed foods are. They feed people bad information(a calorie is a calorie) and then shame people for not "taking care of themselves", all the while polluting geniune research that contradicts them. It's terrible.
Big pharma has totally pwnd the regulations the government enforces on the prescription drug market ensuring they have monopoly pricing power. Why wait for CA to spin up it's own insulin manufacturing industry - just do not prosecute the import/manufacturing and resale of insulin - like it did for medical marijuana in the 90s?
That's second fiddle to the real reason for why we're in the current state of affairs - fleecing the public is much better for the vendors, and it's much better for a politician trying to get re-elected to go along with it.
"Domestic manufacturing" is just a talking point to fig-leaf the real goal.
Reading these comments, I learned about human analog insulin and how it's considered more modern than older, off-patent versions. I was wondering about human analog insulin's patent status, and from here [1] I learned about the practice of patent ever-greening.[2]
TL;DR: "Evergreening is any of various legal, business, and technological strategies by which producers (often pharmaceutical companies) extend the lifetime of their patents that are about to expire in order to retain revenues from them. Often the practice includes taking out new patents (for example over associated delivery systems or new pharmaceutical mixtures), or by buying out or frustrating competitors, for longer periods of time than would normally be permissible under the law."
A relevant quote from the Wikipedia article: "In one study of the prescription drug market, Feldman found that 78% of new patents associated with prescription drugs were for existing drugs."
This is the same argument that giving money to rich people makes the poor wealthier. There’s no evidence of more innovation in larger companies and in fact very often rent seeking causes these big bloated companies to not take risks or generate new opportunities.
„Alec Smith, died in 2017 because he could not afford the $1,300 out-of-pocket price for his prescription once he was dropped from his parents’ health insurance when he turned 26“
What a reality. I‘m glad that I don’t have a life threatening diseases, but I would do everything that is possible to survive. Steal, rob, fraud to come at least up with the money to survive.
I‘m shocked that simply surviving a manageable sickness in a first world country is not a human right.
> because of the Senate’s arcane rules, they could not establish the same cap for private insurance
It looks like one party tried to get this done in reconciliation. If so, blaming “arcane rules” is slanted and makes me wonder what other information the author is twisting.
The reason private insurance was excluded from the bill was because of the "Byrd Rule". The senate parliamentarian gets to rule on and decides it unilaterally. The only reason to do it in reconciliation in the first place is because of the filibuster.
I would say that whole combination is pretty arcane.
To be clear, the parliamentarian is only an advisory role, they don't get to rule or decide anything, only offer guidance which senators then choose to listen to. But they could ignore it (and have done so in the past) or can fire the parliamentarian and pick a new one which is more likely to advise in the way that they want (and have done so in the past.)
It's not the senate generally that is taking the parlimentarian's advice in this case, but the presiding officer, who does get to unilaterally decide (although the have some options).
The rules of reconciliation are indeed arcane. There is a Senate Parliamentarian who makes calls on interpretations because the details are so convoluted.
Sure, at a high level it's simple. But so is "crawl the internet, make a database and match keywords from requests to a ranked list of results."
If the parliamentarian is "overruled" for political reasons, the likely outcome is that the Senate grinds to a halt, not that the majority party gets to pass desired legislation that otherwise wouldn't pass.
The job of the parliamentarian is to interpret the rules and give advice about what is allowed and what is not. Sure, they can be wrong. But if you don't like the rules, change them. Because any self-governing body that isn't following its own rules isn't actually operating. Any legislation the Senate "passes" in violation of its own rules doesn't actually exist. It's an exercise in futility. Both Democrats and Republicans understand this and both parties value an impartial parliamentarian as an asset. It's a job created out of need:
> Charles Watkins had arrived in the Senate in 1904 from Arkansas to work as a stenographer. Blessed with a photographic memory, and a curiosity about Senate procedures, he eventually transferred to the Senate floor as journal clerk. In 1919 he started what became a 45-year search of the Congressional Record, back to the 1880s, for Senate decisions that interpreted the body’s individual standing rules to the legislative needs of the moment.
> In 1923 Watkins replaced the ailing assistant secretary of the Senate as unofficial advisor on floor procedure to the presiding officer. From that time, he became the body’s parliamentarian, in fact if not in title. Finally, in 1935, at a time when an increased volume of New Deal-era legislation expanded opportunities for procedural confusion and mischief, he gained the actual title.
Both sides changed the rules concerning judicial appointments. In both cases this was understood to be a change in actual Senate rules, not a one time override. As demonstrated by the fact that there were many appointments under the new rules without additional votes.
There was little reason to block it and it is hard to imagine why they blocked it given how many people it could help. I tried to understand the logic but most everything I read were just out right lies. I have knowledge of this first hand because my wife takes insulin.
I saw this commend as [dead] and vouched for it, but you should realize that the gripe about "hnews does not like politics" is counter-productive.
I do agree that it's on-topic in this particular thread to have a discussion about the merits of policies like this and that can include highlighting the factions that support or oppose them (and the reasons and/or incentives that might be driving that support/opposition).
This is a failure of the free market. When companies get too big, and no longer compete, they should be regulated. The free market only works when there's a ... free ... market.
That's what I've heard, though I don't any data to show.
In general all medications are the most expensive in the US, often by a lot. For two main reasons:
1. All other countries are to some extent "free riding" on the US market, and refusing to pay full price.
2. The FDA is doesn't approve a lot of things. So many cheap foreign medications are illegal to import. I heard that many forms of insulin are in this group.
Insulin is expensive for the same reasons that epi pens are expensive[1] and why Martin Shkreli could increase the price of Daraprim by 50x without worrying about losing market share[2]. The FDA restricts the manufacture and importation of these drugs. Often there is only one manufacturer who has managed to jump through all the bureaucratic hoops, giving them a monopoly on the drug.
What exactly is California planning to make? The generic version is already available for $25-$30. Why does the state need to get into the manufacturing business?
So we make a law that says a product's intellectual property is protected and cant be copied. Someone in another country copies it, without paying. Then it's legal to import it?
Seems like a very roundabout way when we could just ignore intellectual property laws directly, at home. The same applies to "importing things from Canada." Why the ruse?
Same way people live with themselves working for an Ad companies that tracks people, and social media companies, and every other kind of business that is considered unethical by vast majority of people - by looking at their bank balance and being in denial about the harm they are causing.
One should look at their own employers and see if everything they are doing is ethical.
NOTE: just making a point, I don’t condone what these companies are doing
And it's often treatable through diet and vigorous exercise.
"A weight loss of ~15 kg, achieved by calorie restriction as part of an intensive management programme, can lead to remission of T2DM in ~80% of patients with obesity and T2DM." [ https://pubmed.ncbi.nlm.nih.gov/32690918/ ]
"A novel HIIT-protocol recruiting lower and upper body muscles efficiently improves insulin sensitivity, VO2max and body composition with intact responses in obesity and type 2 diabetes. " [ https://pubmed.ncbi.nlm.nih.gov/36387850/ ]
The caveat, is of course, "long-term weight loss maintenance is challenging."
That's a bit like saying we should defund the police. It's thought provoking and grabs headlines. It even has some merit, but it's ultimately not the solution. Reform the FDA, sure I can support that.
The FDA, from my perspective, plays such a huge and important role in our society and showcases the exact things we need from our government. They are an example of a government entity that mostly gets the job done right, an essential part of our livelihood today.
In 1938, the FDA started reviewing and approving drugs.
In 1960, Richardson-Merrell applied for approval for a drug called Thalidomide, a cancer treatment.
They had clinical trials that included pregnant women. They were rejected six times.
In the UK, The Distillers Company (Biochemicals) Ltd, a subsidiary of Distillers Co. Ltd marketed thalidomide as Distaval, a remedy for morning sickness. Their advertisement claimed that "Distaval can be given with complete safety to pregnant women and nursing mothers without adverse effect on mother or child ... Outstandingly safe Distaval has been prescribed for nearly three years in this country."
By 1962, over 10,000 children (most in west germany) were born with crippling disabilities caused by thalidomide. Over 2,000 died.
Frances Oldham Kelsey was awarded the medal for Distinguished Federal Civilian Service by President John F. Kennedy for rejecting the drug.
I remember reading an archived copy of the FDA press release after they finally approved beta-blockers, a medicine that had been approved and widely distributed in Europe for some ten years. In the press release, the FDA was proud to announce that as a result of their approval, beta blockers would save the lives of an estimated 10,000 Americans every year.
That is to say, the inefficiency of the FDA was, in the words of the FDA itself, directly responsible for the premature deaths of 100,000 Americans. And that was for beta-blockers alone.
I laughed when watching an FDA press conference during covid, where the spokesman said that the agency was streamlining approval measures to get covid vaccines approved faster. A journalist asked if this would negatively impact the safety or efficacy of the vaccine to which the FDA head confidently replied that it would have zero material impact. It makes you wonder, if they are capable of quickly making approval decisions without sacrificing safety or efficacy standards, why is that not standard operating procedure? There are no answers that don't lead one to conclude that the FDA is a bloated, bureaucratic, wasteful mess.
> A journalist asked if this would negatively impact the safety or efficacy of the vaccine to which the FDA head confidently replied that it would have zero material impact. It makes you wonder, if they are capable of quickly making approval decisions without sacrificing safety or efficacy standards, why is that not standard operating procedure?
That's easy. The normal process has multiple trials:
Phase 1: 50 people
Phase 1: 200 people
Phase 3: 100,000 people
Normally, you pass each phase before exposing a larger number of people to risk. More people means you can find rarer and smaller effects, but if you haven't tested on <50 people first then you might really endanger the group of 200 or 100k.
The expedited process tests it on 100,250 people at once. THOSE people are exposed to more risk, but the safety of the vaccine is the same. And because the vaccine was proven safe, those people were not negatively impacted any more than if they had followed the normal process.
> There are no answers that don't lead one to conclude that the FDA is a bloated, bureaucratic, wasteful mess.
Yeah, I mean I'm sure there's a complicated story here... but when the market isn't producing some consumer good, I think it's a good idea to check whether there's some root cause we can fix. Not just throw yet another hack on top of the chaos.
Make pharmaceutical companies work against each other: Have them check their competition and advertise their competitors' malpractice. Having some faceless government bureaucracy delay that process for decades, just hides the truth from the people who need it most.
This "article" has one paragraph dedicated to actually explaining why drugs are expensive, and it says it's because of patents.
It also tries to blur between patents and exclusivity. Exclusivity is usually 3 years (5 for new antibiotics and new chemical entities). Patents are 20. Exclusivity is a very small portion of intellectual property protection. I would call that dishonest.
The FDA does not control drug patents, the patent office does. Abolishing the FDA would do practically nothing to reduce IP protections, but would eliminate all the other things they do, like making sure drugs work and don't kill people.
AFAIK the old school stuff (e.g. synthetic human insulin) is cheap, so I assume that's not the sort they're talking about. Probably they're talking about analogue insulin, which is very expensive.
My fiancée was close to death from a missed diagnosis of Type 1 diabetes. We were extremely lucky that she actually got a diagnosis; A nurse at the oncology ward had a hunch. (Overburdened medical personnel miss diagnoses.)
Her HbA1c long-term blood sugar measurement was literally off the charts. Off the chart on the wall on the hospital, right through the red “DANGER” section. She had lost 17% of her bodyweight and half of her hair.
We have learned the following:
You want a continuous glucose monitor (CGM), and an insulin pump, with rapid-acting insulin.
You do not want long-acting insulin. Especially not insulin glargine. It is a dangerous form of insulin: It is injected as a blob of insulin (“bolus”) under the skin. It’s supposed to stay in the place and slowly fritter and diffuse into the bloodstream. This effect is due to crystallization of the modified insulin amino acid chain in the pH level inside the body. It’s clever. However, if insulin glargine happens to go into a blood vessel, it works pretty much instantly. Then it is not long-acting at all. The subcutaneous environment is… living tissue. There are capillaries. It can and will go into directly into the bloodstream at some point. For some reason. At injection time, or due to bumps and jostles and physical pressure. Then there are no brakes on it. 24 hours’ worth of active insulin can go into the bloodstream. Then every cell in the body is signaled hard to pull glucose from the blood – all the flesh in the body rips the sugar out of your blood, leaving too little for the brain. People start losing consciousness in minutes, csn pass out, and may die.
Insulin degludec is another long-acting insulin, one which is acceptable in this regard. The bolus stays glommed together due to polymerization of the insulin so it’s more robust. It also has molecular brakes on it kind of – if it does go into the bloodstream, it attaches to albumin in blood plasma and doesn’t become active all at once.
However, using rapid-acting insulin in a pump is strictly better because this replicates the insulin oscillation of the pancreas. “[The pancreas’] basal insulin level is not stable. It oscillates with a regular period of 3-6 min. After a meal the amplitude of these oscillations increases but the periodicity remains constant. The oscillations are believed to be important for insulin sensitivity by preventing downregulation of insulin receptors in target cells. Such downregulation underlies insulin resistance, which is common in type 2 diabetes.”—https://en.wikipedia.org/wiki/Insulin_oscillation
The insulin pumps work this way. They pump the insulin with a rhythm. It’s easier to control the blood sugar and you need less insulin. It’s crucially different and much better for long-term health and quality of life.
The most important things are a good blood sugar sensor (continuous glucose meter or CGM), and a good pump with a good user interface. We haven’t tried one of the closed-loop automatically controlled pumps that reads from the sensor and autoadjusts, but it’s clear from the problems people have with badly designed pump that a good “semiautomatic” pump is better than a poor and unpredictable sensor-feedback-controlled automatic one. These have issues like sometimes cutting out without giving clear warning if blood sugar is high, and the blood sugar target range can’t be adjusted low enough (liability issues afaik) so people tend to stay at too high blood sugar levels which do long-term harm. I do assume that a good automatic pump is magic.
Also, glucose metabolism and inflammation are intimately related, which ties into the vascular system. There is a lot more actionable science out on this than most doctors are aware of. (Overburdened medical personnel are unable to keep abreast of scientific developments.)
This is sweeping a lot of problems under the rug. Many US governments are so disfunctional that it's unclear that they could succeed at European-style public housing.
An analogy: just because Japan has a very good high-speed rail network doesn't imply that a new one will succeed in the US. In California it's an open question whether it's going to succeed in the end. You can't assume the US way of doing things like that will do as good a job as other countries on some things, because the culture and politics are very different, and sometimes that means we screw it up.
California has a vast and robust sprawling network of socialized transportation, the budget for which has doubled in the past 2 years to consume 7% of the annual state budget. Think I am talking about high speed rail? No, just the freeway department, which spends 40x more every year and the economic sustainability of which is never even obliquely questioned.
In short, California has plenty of appetite for socialism, as long as it is the kind they want.
Am I reading this right? Are you saying that each decade, the California freeway department multiplies their budget by a quadrillion? If their budget was $1 in 2013, they would now be spending more money than there exists in the world? I'm going to request a source for that.
> A master of complex politics at home, Bismarck created the first welfare state in the modern world, with the goal of gaining working class support that might otherwise go to his socialist opponents.
In the US (a nation of 320,000,000 people), around 5 people per year die from this[0]. On the list of causes of death that need attention, this one is considerably lower than lightning strikes (which kill ~20 per year)[1].
Is it a problem? Sure. Is it an argument for reorganizing our economy? Hardly.
> A master of complex politics at home, Bismarck created the first welfare state in the modern world, with the goal of gaining working class support that might otherwise go to his socialist opponents.
It looks like your account has been using HN primarily for political and ideological battle. Could you please stop? It's not what this site is for, and destroys what it is for, so we end up having to ban accounts that do this—regardless of which ideology they're for or against.
the constraints of cited issues (affordable insulin, housing) are due to cartel-like behaviour from stakeholders in the market.
It is not a characteristic of (freemarket) capitalism in itself (like, the rest of the world make it work), but a concentration/tyrrany of powers (patents, regulation, lobbying) and a disregard of human life/health in society.
These are not factors that disappear in a socialist/comunist framework unless one is "government from the people" naive.
A "simple solution" would be to make patents on critical things to be "opensourced", licenseable in automatic to anyone interested in exchange of a % fee on sales to patent-holders, making still competitive for Original-inventors to produce things at a competive advantage while keeping prices for End-Users "honest" due to production competition
Confusing. The people saying "The Nordic Model isn't socialism!" are the people who are responding to "No, that's socialism!" Saying that the nordic model isn't socialism is a response to those who oppose it by saying it is, an attempt to persuade anti-socialists to chill out.
> Saying that the nordic model isn't socialism is a response to those who oppose it by saying it is, an attempt to persuade anti-socialists to chill out.
Could someone against the idea of providing food for children at school explain their position? I'm interested to hear why you think children should go hungry if their parents don't give them cash to bring to school.
I think I can do a decent job of steel-manning this- I might be a bit unfair because I think it's rather morally reprehensible and deeply harmful (and also suspect these are only the stated motives of folks pushing this idea), but I can try.
Everybody generally agrees children going hungry is bad. What we're really arguing about is whether the government should be spending taxpayer funds on feeding them.
In fact, because the overwhelming majority of people see child hunger as bad, private charity would step in to feed those kids who aren't fed by the state. This is better in two ways: first, it's more voluntary (instead of "donations" being compelled by force), and second, private (market-driven) charity can be more efficient than a state monopoly.
So it's not that kids should go hungry, and I (n.b. this is me in-character!) am a bit surprised that you think I seriously believe that. Rather, kids necessarily go hungry if nobody feeds them, and the debate (OOC: note i'm deliberately reframing the harm here as a natural thing!) is really over who should step in if the parents, the natural caretakers, aren't able to support their child. Should the government use taxpayer funds to do so, or is voluntary charity a better option for everybody?
Additionally, there's a moral hazard here where the state effectively subsidizes having kids that a parent might not be able to take care of on their own.
The keyword is "immanent justice" and its twin sister "unconditional grace". Bad things happen to those who deserve them, and also, since bad things do not happen to you you are counted amongst the good guys and are visibly favoured by the Lord God who looks out for his own. If that sounds sick in the head, that's because it is.
As someone who grew up in country with such policies it is easy - it creates bad incentives for school cafeterias. They can push quality of food down, because they have monopoly for government food money. So the food is barely eatable, you could buy much better food over the street (or just eat at home), but then you have to pay the full price.
Also it discriminates against people with strong dietary preferences. E.g. if you are a vegetarian, and school cafeteria does not offer vegetarian food, it is no government food money to you.
Also, fair question is not 'free food in school cafeterias or not', the fair question compares equally expensive alternatives: 'should this government money go to parents as child benefits, or to school cafeterias for free food'.
The premise is bullshit, schools in America always give the kids lunch whether or not they have money that day. Kids who forget their money still get fed, the schools insist on it. Even if the kid pleads that he's just not hungry today, the school will put a tray of in front of him anyway. If the kid isn't getting free lunches already through the National School Lunch Act (which gives free or reduced price lunches to 30 million kids a year), then the money they owe will be recorded and their parents will be asked to pay it later. If the parents can't pay, the kid will be signed up for free lunches reimbursed by the federal government. But at no point does the school not give the kid a lunch.
It's sort of baffling that people could be angry about the mention that this sort of thing exists when there are school districts that not only racked up gigantic deficits from parents but also refused to allow third parties to pay off those deficits. It's clear that this was never a financial issue for those school districts. They wanted these people to individually suffer for the sin of being poor.
I can second the latter one since living in a tiny apartment here costs 20k a year before utilities, and that's a lot of money when my family doesn't have a 10x developer making 100k
For context: the patent on insulin was sold in 1923 to the university of Toronto for one dollar because the inventor felt it was unethical to use this invention to make egregious profits off people who had no alternative. This is 100 year old technology. It's not a manufacturing, regulatory, or technological issue. It's just monopoly pricing and greed.
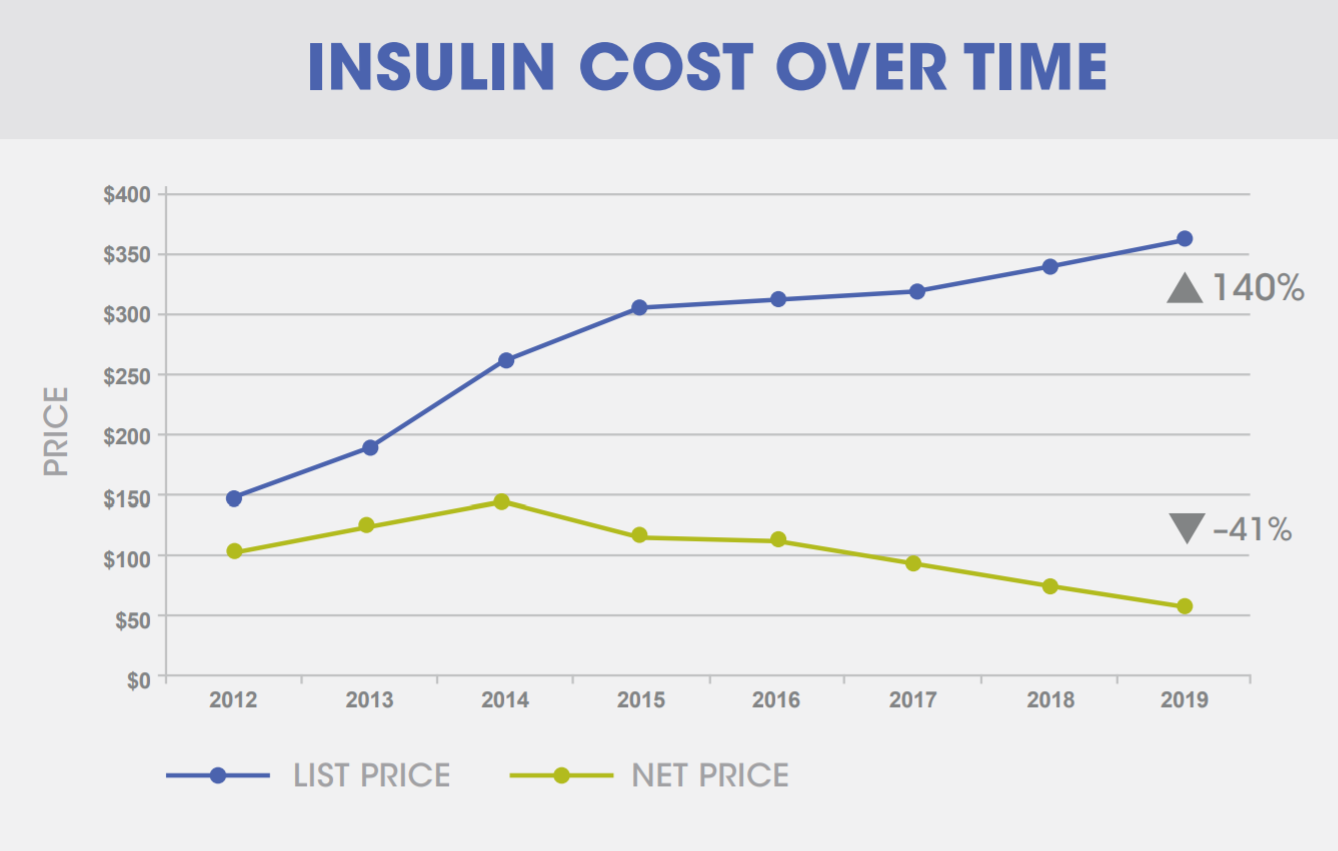{kind=link}
> With California leading the way, a handful of states are considering trying to disrupt the market for essential medications, starting with insulin. The plan would be to manufacture and sell insulin themselves for a price that is roughly equivalent to the cost of production.
I feel like I'm missing something here. My understanding of why insulin is so expensive: laws are created and enforced by the government preventing people from competing in the space.
If you try to make your own insulin, and you take it to market with 3rd party analysis and certification of it being medical grade (and safe) insulin, you'll start seeing an escalation of the state against you. First angry letters from lawyers and eventually, if you continue head strong and ignore everyone telling you to stop, government officials (possibly with guns) will come and forcibly shut you down.
Is California just going to ignore these laws? How will the state not be liable for damages when individuals are?
I'm all in favor of revoking the legal structures that pick the winners in this market. It seems like there are plenty of people passionate in this space that would/could make insulin at near-cost if permitted to.
It's just that, by my understanding, it's the government that doesn't permit them to. It's weird that people in the government (at the state level) are stepping in to do what people in the government (at the federal, but possibly also the state level?) won't let people in the market do.
Edit: substituting “intellectual property laws” with “laws” as it seems there’s more to it than just IP.