I have a friend in southern Ohio who is an ICU doc. They’ve been dealing with +140% occupancy for the last few weeks. Staff shortages in their hospital are due to people leaving the field entirely (either worn out, tired of patient abuse, or actually dead). Vaccine mandates had almost zero impact.
To be clear, the vaccine mandates for healthcare staff had little to no impact on actual care. Very few professionals were unvaxxed and even fewer left/were dismissed as a result of not vaxxing (i.e. they got vaxxed). The staffing is low because providers are leaving or have left the field due to horrid conditions. However, the real issue here is that the bed count didn’t go down just because there was no one to cover… Hospitals in many places are simply being inundated with patients (mostly unvaxxed).
I think that they are commenting specifically on the reasons for the staff shortage, in response to the popular claim that people are quitting their jobs over the vaccine mandates.
is this 9 out 10 stat real ? Where i live, govt has tried to spread those numbers, but they were actually incorrect:
That 9 out of 10 number they talked about was actually the chance of ending in hospital if infected depending on vax or not ( aka : you're 9 times more likely to end up in hospital if you're not vaxed)
But hospitals were actually in majority filled with vaxed people.
In my hospital (located in Ohio), yes it's about that. We are seeing the overwhelming majority of deaths from unvaccinated individuals. I don't have the exact number in front of me but I believe before I logged off on Friday it was somewhere in the upper 90%s. Like basically every other hospital system in the state we've been above capacity for months.
From what I've read the hospitalization ratio between vaxxed and not tends to mirror the death ratio between the two. Within ~10% or so. E.g. 9:1 might become 8:1
Beyond Covid, this is a very scary situation that will only get worse as the numbers continue to climb in the region. You do NOT want to need medical care of any kind right now in NE Ohio.
We just canceled our trip to see family in Cleveland as a result. My youngest has a bad cold (PCR negative) but if that were to get passed to my elderly parents or asthmatic nephews, things could escalate quickly.
It almost doesn’t matter how severe Omicron cases are if the net result is hospital overload.
Training of COVID-only staff, separation of COVID patients into dedicated hospitals, etc. It's all been done before. Many COVID patients just need basic attention and oxygen, the ones with really complex needs tended to have other serious illnesses anyway.
I don't consider the admins to be in charge, I am thinking the head of health departments: they should have massively upped beds, machines and so forth and improved working conditions, including a massive pay boost.
If we cared about up front treatment as much as we cared about vaccinations and stopped seeing one as preventing the uptake of the other we'd see a lot less hospitalizations.
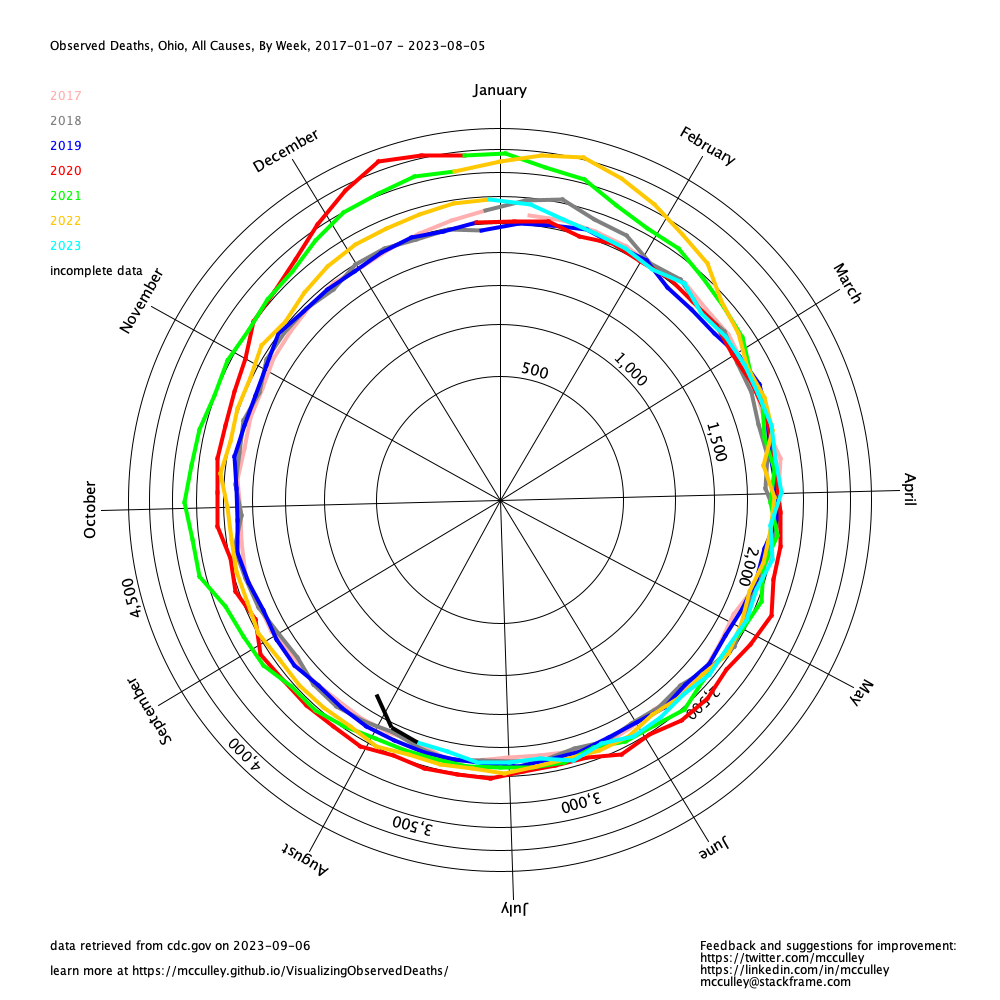
I am a little skeptical about the claims in the article that Ohio COVID deaths are higher in 2021 than in 2020. I have been building tooling around the CDC excess deaths reports [0]. Ohio looks like it did not have the same peaks in 2021 as it did in 2020 [1]. There would have to be 11,778 more deaths recorded at this point to catch up to 2020.
Certainly the situation is unacceptable and terrible. But I am not convinced that it is much worse in 2021 than in 2020.
It does if you're willing to be a travel nurse and work on covid floors. I've been hearing $6000/week numbers being thrown around (and some nurses are picking up two contracts at a time!). It's insanely shitty work right now (surrounded by people dying left and right and understaffed on top of that, but the pay is good...).
Have to incorporate a premium for the travel nurse job being not in your home office, income being more volatile than a salaried job, and travel nurses are independent contractors so they have to pay for housing/health insurance/taxes.
The $6k per week easily comes down to $3k per week or less of comparable W-2 income, which you can come close to or surpass doing virtual scrum meetings with none of the income volatility of nursing nor the messiness or risk of being infected or attacked. And not seeing your family/friends after work.
The travel job typically has housing built in too and often per diems. So probably closer to 4-5k equivalent! But quality of life isn't great to your point. Software is the objectively better job there unless you're really passionate about nursing!
I would appreciate any help in squaring things like this story with seeing 50k plus in (indoor) sports events with no masking or other remediation measures. And they’re in the same or adjacent states. Is it merely that they’re tolerating the deaths and sickness as less important that their inconvenience?
Uhh, delta and omicron are contagious to doubly vaxxed. And spreadable by these people as well. You’re gambling to some degree that you won’t have a problem or you won’t be around those who are at higher risk. I hope it’s a good gamble with omicron as this will greatly facilitate switching to endemic but nobody’s sure yet.
The risks of someone my age having serious COVID issues are rather low. I am also fully vaxxed on Pfizer and don't have major underlying health issues. I'm perfectly accepting of the any personal risk because the risks are extremely low. In fact, I had COVID recently (kids caught it at school and brought it home), and my symptoms were very mild and didn't prevent me from working of functioning close to normal. Of course, we all followed proper quarantining guidelines and did not have contact outside of our home with anyone during that period.
If other people who are at higher risk have not chosen to appropriately mitigate their risks with the numerous tactics at their disposal, such as vaccination, masking, social distancing, etc. than I do not feel much of a duty to avoid being around them, if they are going to be at places I want to be.
The organizations that employ healthcare workers, and indirectly the organizations that pay for healthcare, do not want to pay sufficient wages to incentivize people to work in the roles needed to provide the level of healthcare expected by the population.
Instead of fixing the remuneration so that people are incentivized to work in healthcare, the easier solution for leaders is to “draft” who chose to be eligible to be drafted in emergencies and have them work. In reality, this is simply displacing healthcare workers from elsewhere.
It is leaders of today destroying trust in emergency organizations, protocols, and structure to avoid paying higher wages. Why would anyone sign up for national guard when your role includes having to work because of insufficient wages causing lack of supply of labor?
This really doesn’t have anything to do with wages. Healthcare staff just don’t exist in the quantities we need right now.
It’s a worst case scenario with a bunch declaring early retirement, even more changing professions due to COVID trauma, and lack of proper pipelines of staff.
This has everything to do with wages. Nurse to patient ratios have been getting smaller and smaller for many years now. It is a common topic in medical forums.
It is combined with a worst case scenario, but it is compounded by the fact that a parent or young person is going to look at Mar 2020 and decide to not go into nursing because all they got was a sign saying they were heroes in exchange for working with an infectious disease, while many others got to sit at home on their computers.
The situation for nursing homes is even worse than hospitals and nurses. It actually terrified me, even pre pandemic, to think about the level of care I would get if I had to be in an assisted living facility being taken care of by someone earning $12 per hour also taking care of 19 other people. I would rather opt for suicide.
It matters in the grand scheme. The pandemic started 21 months ago, and there is still insignificant movement in wages.
Also, if you offered 20-30x, the people would exist (for your facility). And if you offer 2-3x market rate and cannot attract people, then not only is x not the market rate, but 2-3x is not either.
The article says that about 150 of the 1050 troops deployed are medically trained. Most will be providing support services where needed.
The national guard exists to answer the call of the state governor for all sorts of things. You’ll also see them deployed for state emergencies like a hurricane or tornado.
Think of it as a quick to mobilize population of volunteers that are trained to do various things.
Yes this is one of the main benefits of having military type orgs available even if not in conflict - you have a group of proven competent people, trained to execute orders that you can deploy into a variety if situations where people power is useful/important. The British Army were used for the 2012 Olympic as marshals etc as G4S messed up the preparations.
FTA:> “Earlier in the pandemic, our concern in our hospitals was about beds, was about space, today is about personnel,” DeWine said. “22 months. 22 months of this pandemic has taken its toll on our health care workers, and that is certainly, certainly understandable.”
> Of the 1,050 national guard troops being deployed, about 150 are medically trained personnel who can assist in helping patients. DeWine insisted that he and Adjutant General John Harris have worked together to ensure the deployment won’t mean pulling people away from a hospital day job to go work at a different hospital. The remaining 900 troops will be tasked with support services.
> “They will do many things to help the hospitals in this time of great, great crisis,” DeWine said. “It will involve transport within the hospital, food and the environmental work that goes on in hospitals and is so very important every single day.”
This is not unique to the USA, e.g. in the Netherlands the army assists in testing and vaccination campaigns [1]. This is just common sense, those organisations have a large number of people (who in peacetime have not much more to do than exercise and maintain their equipment) who are trained to act in a short times notice and can deploy facilities which are not available to civil authorities.
Because our hospitals are over capacity - specifically well over 100% nurse to patient capacity - the guard members will likely be helping with all of the non-medical work nurses would normally do in non pandemic times. Stuff like cleanup, re-supply of rooms and supply closets, maybe some check in work that sort of thing.
Probably because procedure volume was down, so they canned people who they could. And then got caught off guard when demand increased again suddenly. Same thing happens over and over in manufacturing.
It's inherent when quarterly numbers trump long term stability. If managers are only incentivized to meet short term numbers, they make decisions that are detrimental to the future to meet present-day goals. Our financial markets reward this (though there's a question about why they do this that's open in my mind, as most of the money in the market is invested long-term!), so it trickles down into managerial metrics.
There's a huge bottleneck in training and education of the licensed professionals involved in nursing.
To have a 'truly free market', there wouldn't be government licensing (a similar role would likely be carried out by third party certification).
I don't think that eliminating licensing would improve anything, but the regulation of nurse training absolutely needs to be included in the discussion of the problem.
> if there's a truly free market solution to this issue with hospital staffing.
You are seeing it happen. People do not accept current labor prices for healthcare work, politicians come under political fire for not providing sufficient level of healthcare, politicians increase funding to healthcare to increase pay, possibly requiring increasing taxes if they cannot figure out how to punt them to future generations.
Or insufficient number of voters want to direct more resources to healthcare to those that cannot afford it out of their own pocket, and they get less or lower quality healthcare. Maybe society decides it is not worth the cost of supporting people past 90, or even 80.
There's plenty of people willing to work at the offered salaries, there is a structural problem in the licensing process preventing them from doing so.
A case can be made for doctors who have limited residency spots effectively capping new yearly supply, but what possible argument could there be for nurses other than nurse pay is not high enough to attract more people to nursing?
People changing bedpans get paid $10 to $15 per hour in many states, who wants to do that unless they have zero other options?
How do you know the people not accepted would have made desirable nurses? Surely one would want some minimum standard for the people poking you with needles and administering your healthcare/medicines.
> The trainers that are training are not well compensated.
I don't know it, but I sort of take it as a given that the marginal rejectees are going to be roughly as capable as the marginal acceptees. It's not really an aggressive assumption.
And it isn't just an insufficient pay scenario. Hospitals just pass on the high cost of nursing to patients instead of subsidizing training programs. Patients don't see the supply as part of the cost problem and don't demand that more money be devoted to education.
Yes, the feedback mechanisms get
quite complicated because 80%+ of people cannot not afford the level of healthcare that they receive.
But the root of the problem remains the disparity in people’s expectations of the services they will receive with the amount those service providers are getting paid.
Health care is so regulated that the word free market doesn't make any sense.
A truely free market solution would be to train people specially to deal with COVID-19 cases and build a specialized hospital to deal with that. It would also bring the cost down.
Any kind of efficient resource allocation relies on accurate predictions. No matter what system you use, free market or otherwise, if reality is constantly defying prediction, or changes too quickly, allocation won't be great.
Some got fired. Some quit and found different, better paying jobs. The reality is that being on staff, working at the bedside in a hospital is a hard job with mediocre pay. But hospitals will give docs huge bonuses and pay travel nurses 2-3x what they pay nurses already on payroll. My wife was an RN at a major pediatric hospital and took a job at a private practice. Much easier job, closer to home, better pay. The hospital called her a month after she left and offered a 5k rehire bonus. Thank you, but no.
I'm near Dayton, Ohio. We had lots of protesting back in August by self-proclaimed medical personnel who were unhappy with vaccine mandates. How many of these people were actually medical personnel, and how many actually quit due to their opposition to the mandate isn't clear, but the feeling I was left with was that a significant number of local medical personnel were unhappy with the mandate.
Mandates and threats are counter productive. Lotteries are associated with waste and make government seem desperate. If the government was really wanted to encourage vaccinations it would provide a fixed compensation.
> It has a more dangerous risk profile than the previously accepted vaccines
Is there compelling research that shows this is actually true? There is elevated risk of heart inflammation, but in my understanding that is not an unprecedented vaccine side effect. I haven’t seen an in depth comparison to established vaccines though
As for neurological side effects, I just read this a morning this large study from uk comparing risks between the conventional platform ChadOx, the BioNTech mRNA platform, and actual coronavirus infection. The two vaccine platforms seen at least on par with each other, and both favorable to infection
I came across an amazing resource the other day that provides data driven insights specifically to Ohio's covid situation, and I'm surprised not to see it in this article.
The key here is the words "this year". Most of the deaths this year occurred earlier in the year when vaccination was not available. I've tried finding the data on the state and CDC website a couple of times throughout the year to no avail. I would like to see the trend right now or at least the past couple months data.
When Ohio released it's "breakthrough" dashboard, I thought it was misleading as well since it included all of 2021 and the vaccine wasn't available to all adults until mid-April or so. Because of that, I started recording the weekly snapshots for a few weeks but lost interest. Since I was capturing weekly, you could just look at the new numbers. Here's what my data showed for Ohio:
Between Sep-15 and Oct-27, there were 2899 COVID deaths. Of those, 2625 were unvaxxed or partially vaxxed and 274 were fully vaxxed. So fully vaxxed deaths were about 9.5% of COVID deaths during that period. I stopped capturing weekly data at that point.
I just went and looked at it again with the most updated numbers and from Oct-27 when I stopped recording weekly data and today, 92% of Ohio COVID deaths are unvaxxed.
Given all that, I don't think starting at 2021 is all that misleading at all. Ohio's fully-vaxxed rate for adults is around 65%. Even assuming it was closer to 60% in the fall, you have 40% of the Ohio's population accounting for 90%+ of its COVID deaths.
Lol on lumping an entire segment of the population who disagrees about one particular matter into an entire separate group who also happens to agree on this one particular issue. Better provide a link to a BLM site too, because they also agree on opposing vaccine mandates.
I can't believe people are downvoting your post. If they want to influence someone, understanding them is how to start. Saying "I'm right, you're wrong" provokes resistance. They want others to change to save lives but aren't willing to change themselves to save lives. Listening and making people feel understood goes a lot farther than facts, numbers, and orders.
Because some people have already had COVID, received natural antibodies as a result, and are relying on time-tested science, logic, and intuition in their personal decision to not also get a set of shots + [x] boosters so they can be “safe”. By the way, do me a favor and solve for x in the above equation! And solve again a year from now. And again 5 years from now.
I completely agree that having been infected with COVID should excuse one from vaccine mandates, at least within some time frame. However, that isn't why most of the unvaccinated are unvaccinated. Only a few million people had been infected with COVID in the U.S. at the time the vaccine was released, around 1% of the population.
Not everyone goes to the doctor for a scratchy throat (primary symptom of Omicron, by the way), and as a result a huge number of data points are quickly excluded from that “1%” stat.
We can say with fairly high confidence that the natural immunity rate is fairly low due to the infection rate of the unvaccinated vs. the vaccinated. If any significant portion of the unvaccinated had natural immunity, then the gap between the vaccinated and the unvaccinated would close since natural immunity actually confers more protection.
Influenza, tetanus, TBE and polio vaccinations also require repeat shots from time to time - and there are certainly more as these are only the ones that I can remember off the cuff.
In the case of the flu, the jury has always been out in it’s effectiveness due to the seasonal variation (the flu shot (notice how that’s never been called a vaccine, for good reason) is based on previous year’s strain.
Lumping that in with the rest of the diseases on your list where a vaccine can and does provide true immunity is a massive case of apples and oranges.
Of the many people who have told me that they have had COVID already, none have donated blood and received a free antibody test. I donated blood three times between the start of the pandemic and getting the first vaccine. I got three free antibody tests.
Most of the unvaccinated that I talk to who claim to have had COVID but won't give blood say they are scared of needles. So it makes sense they are scared of getting the vaccine.
I don’t understand your point. It’s a vaccine, you get vaccinated, your body produces antibodies, your risk of catching the disease goes down, your risk of ending up in hospital nearly disappears
Anything is possible when you decide to change the definition of what something means. The CDC used to define “vaccinated” as “the act of introducing a vaccine into the body to produce immunity to a specific disease.” They changed that key word in the definition to “protection”, so sure if you move the goalpost on what something is, you absolutely can call this a “vaccine” and not an MRNA treatment!
When push comes to shove, 99.x% of healthcare professionals get it. So we're taking a rounding error in staffing. The problem is how many nurses just got up and quit in the past couple years
A lot of these nurses will not go back, pay raise or not. Sister gets inundated with offers 2x to sometimes 3x her current pay, but she'd rather avoid the stress. Many of her former coworkers have also moved on.
How about 4x, 5x, or 6x pay? I would throw my own hat in the ring for $800k/year.
The job is not hard in the sense that only a few people in the world possess the capacity to do it.
Society needs to decide what it values more - quality bedside care in hospitals to people that cannot afford to pay out of pocket, or paying people a lot to sling spreadsheets to each other from the comfort of their home.
Why would it not? Staffing for healthcare workers had been barebones for a long time before Covid.
Obviously, the acute situation of today, I would not count. But when managing a society, and you pay rock bottom prices and lower quality of life for a couple decades to limit supply of healthcare workers so that you are running on razor thin margins, then the future where lack of healthcare workers in cases of emergency are inevitable.
Because you are allowed to do the work if you are licensed. The cost of a nurse is conditioned on the licensed supply, not the willingness of Joe Programmer to do it for $800,000.
At the moment, if you chose to go into nursing, the choice wouldn't matter, because the licensing pipeline is full!
I agree with you that in the current situation of 1 to 2 years, my choice does not matter.
> The cost of a nurse is conditioned on the licensed supply, not the willingness of Joe Programmer to do it for $800,000.
The supply of a nurse is conditioned on cash flow prospects. If nursing paid more and had a history of having decent pay to lifestyle ratio, then there would have been more supply of nurses.
That was my underlying point. All of these problems are a problem of society’s willingness to spend x resources on y cause, and it should get very interesting as the population pyramid gets much older than ever before in the world’s history.
For example, I am not enthused at directing a lot of society’s resources at sustaining 80+ year olds while our kids are not well taken care. But that is a different topic.
The only reason this disease was such a big issue was because hospitals were constantly operating on slim margins in the first place with ICUs regularly filling up in winter. How about some breathing room for all involved?
The sad thing is, this kind of money oriented, employee exploiting attitude is just as prevalent among academic and non-profit hospitals as the for profit ones.
Mandated vaccines in healthcare settings aren’t a new demand though. It’s more like a certificate that takes an hour is added to the list of 8 other certificates you need to maintain.
{kind=link}