I'm glad the OP made the correct decision in this case and hope they get well soon.
> the assumption I had a minor cold
> the loss of smell was total
Since there does seem to be a messaging problem about the reliability of testing, I think it's worth emphasizing: if someone has symptoms of COVID, they should proceed as-if they have COVID. CDC guidance[1] is to isolate if you have a positive test OR if you have symptoms.
To do otherwise is to gamble with the health and lives of the people they meet, and the people those people meet, and so on. It may prove almost impossible to show who caught COVID from whom, but that doesn't mean that ignoring guidance won't lead to deaths. A statistical death is still the death of a real person, even if we can't put a name to them.
To be clear, the order of events was such that I did not have loss of smell/taste at the time of the rapid tests. There was no indication at that time of anything that wasn't completely consistent with and expected from a cold, and I even encountered resistance when I tried to get tested prior to the tell-tale loss-of-smell symptom appearing (hence the rapid tests only at that point). I had a mildly uncomfortable phone call with an urgent care center where they discouraged me from pursuing testing because they didn't think I had enough symptoms.
I knew exactly from whom I had contracted whatever illness I had, and that person had also tested negative for COVID (upon further questioning, their test had also been a rapid one, and they too had not been informed of its unreliability for any negative determination).
> There was no indication at that time of anything that wasn't completely consistent with and expected from a cold
Unfortunately, I think these days symptoms of "just a cold" are enough reason to self isolate for long enough to reliably get through the Covid incubation period - which locally (Sydney .au) has been reported to occasionally be as long as 10 days or more.
The USA currently has nine million active cases. I actually think at this point if you have cold symptoms it may be more likely you have covid than a common cold.
(Though maybe someone has data in cold cases to clarify the cross over point)
> The USA currently has nine million active cases. I actually think at this point if you have cold symptoms it may be more likely you have covid than a common cold.
Your intuition is wildly off-base here. Nearly all of us catch at least one cold a year, mostly during the winter months. There are, quite literally, hundreds of millions of colds a year. There's also ~half a dozen viruses in circulation at any given time that cause cold-like symptoms, vs. one for SARS-CoV2.
The steps we are taking to reduce COVID spread also reduce the spread of the cold. I would be absolutely shocked if we don't end up having our lowest impact cold and flu season in decades this year. That isn't to say the grandparent comment is correct, just that you can't really use a comparison from prior years as an indication of how many people will get a cold this year.
In the first 6 months of 2020, Australian influenza deaths were down over 90%, attributed to Covid anti measures - mostly increased hand washing/sanitising, social distancing, and school closures.
If we assume that's representative of a 90% reduction in flu and cold cases (not guaranteed, but probably a reasonable estimate to reason about), then perhaps instead of "hundreds of millions" of cases, it might be down to "tens of millions of cases" of cold/flu. So maybe 9 million Covid cases means any cold/flu symptoms are somewhere between 50% and 10% likely to be Covid - a virus currently killing ~1% of the people it infects.
I am certain the prudent thing to do in 2021 is assume _any_ cold/flu symptoms are likely to be a virus that's quite capable of killing you (and/or the people around you) and act accordingly until you are 100% certain it's not. (Which probably means 2 negative PCR tests ~10 days apart.)
> The steps we are taking to reduce COVID spread also reduce the spread of the cold.
...and cases are going up, so it's probably safe to assume that there are lots of colds being transmitted, as well. And as I said, there are many cold viruses in circulation, at all times.
Even if you believe that "the steps we are taking" are working, you have to assume that they're disproportionately effective for the common cold in order to make the statement the OP was making. Say what you will about SARS-CoV2, but it's more-or-less like any other respiratory virus in terms of transmission characteristics. There's no particular reason to believe that anything we're doing would stop rhinovirus or RSV, but not SARS-CoV2.
This doesn't follow at all because you are comparing the current state of laxing COVID precautions to the previous state of near zero cold precautions. For example, tens of millions of people are currently working from home and the workplace is one of the primary places colds spread. If we treated COVID like the cold we would already be on the other side of the pandemic because it would have already ripped through the population and millions would be dead.
> This doesn't follow at all because you are comparing the current state of laxing COVID precautions to the previous state of near zero cold precautions.
I am not. There are, right now, 5-6 cold viruses in common circulation. There is one SARS-CoV2 virus.
Nothing we are doing would be expected to suppress other respiratory viruses, but not this one.
>I am not. There are, right now, 5-6 cold viruses in common circulation. There is one SARS-CoV2 virus.
Yes you were. In your first comment you said "Nearly all of us catch at least one cold a year, mostly during the winter months. There are, quite literally, hundreds of millions of colds a year." Those are numbers in a normal cold year. This isn't a normal cold year.
>Nothing we are doing would be expected to suppress other respiratory viruses, but not this one.
I'm not sure where this line of argument came from as no one was arguing against it. The assumption is that these COVID precautions are equally effective against the cold, flu, COVID, and other similar respiratory diseases. This will lead to a huge drop in those non-COVID diseases as the precautions we are taking are so drastic compared to a normal year.
> Yes you were. In your first comment you said "Nearly all of us catch at least one cold a year, mostly during the winter months. There are, quite literally, hundreds of millions of colds a year." Those are numbers in a normal cold year. This isn't a normal cold year.
You can divide the number by any factor you want, but there are still ~6x the number of viruses out there causing colds. Even now.
>there are still ~6x the number of viruses out there causing colds
The variety of viruses is totally irrelevant to the original question of what are one's odds of having COVID based on having cold symptoms. The only piece of information that matters for that are the aggregate numbers and aggregate numbers from previous years are misleading.
> The variety of viruses is totally irrelevant to the original question of what are one's odds of having COVID based on having cold symptoms.
It is an essential factor, unless you make the (implausible) assumption that we have essentially eliminated all other respiratory viruses except for SARS-CoV2.
I like how you cutoff the my quote at the exact point that shows you how you are wrong. As I said "The only piece of information that matters for that are the aggregate numbers".
Whether there is 1 version, 6 different versions, or 1 million different versions of colds is irrelevant to your odds of having COVID when you show symptoms. What matters is whether there is 1 person, 6 people, or 1 million people with colds. The variety is meaningless. What matters is the aggregate number of cases.
> The variety of viruses is totally irrelevant to the original question of what are one's odds of having COVID based on having cold symptoms. The only piece of information that matters for that are the aggregate numbers and aggregate numbers from previous years are misleading.
It is an essential factor, unless you make the (implausible) assumption that we have essentially eliminated all other respiratory viruses except for SARS-CoV2.
I catch colds roughly 7-8 times per year. It sometimes feels like I have cold symptoms more days than I don’t. I currently have cold symptoms. If I had to isolate every day I had a cough, sore throat, congestion, or sneezing, I’d be under house arrest most of the year. I think it’s vitally important that we have accurate COVID tests that can definitively distinguish a case of the cold from a case of COVID.
At the end of the day everything is a judgement call. In this case I believe you're an outlier, guidelines are usually structured for the general case. Should you specifically treat every cold like it could be COVID? Maybe not, but should somebody else who gets sick only 1-3 times a year treat every cold like it could be COVID? That seems a lot more reasonable.
Not to mention it is wise and courteous to stay home and avoid exposing yourself to lots of people when you are sick regardless of if its COVID or not.
Not everyone can afford to stay home with minor illness. Not everyone will be employed if they stay home and can't "cover" their days off with measly 40 hrs a year of paid time for such purpose ( if they have any paid time at all).
This issue existed long before COVID. COVID is spreading partially due to this issue. Many people have no choice but work to avoid homelessness and/or hunger.
You should be tested for primary immune deficiency, based on the frequency of your colds alone. If you do have primary immunodeficiency, it is treatable with subcutaneous immunoglobulin, in most cases. Either way, it is treatable.
I am personally on subcutaneous immunoglobulin for two rare immune-mediated neurological diseases, and I have not had a cold in over 3 years, when I would get them a couple of times per year. It helps tremendously.
These are the 10 warning signs of primary immune deficiency in adults:
Adults
If you have two or more of these signs, speak to your doctor about a possible Primary Immunodeficiency.
1. Two or more new ear infections within 1 year
2. Two or more new sinus infections within 1 year, in the absence of allergy
For the broader point, regardless whether or not someone is more likely to have a common cold or COVID given the same group of symptoms, I think the point stands that if someone has symptoms consistent with COVID they should proceed as-if they have COVID -- especially given the current case rate in US.
Are you sure? Do nearly all of us catch a cold _this_ year? I know the flu is way down this year due to covid-related behavioral changes. I'd be surprised if common colds are unaffected.
I agree with you, and that's largely why I wanted to share my story -- to illustrate that even without any tell-tale symptoms and multiple negative test results, you can easily still have COVID.
Thanks for sharing your story, it's useful to hear anecdotes. I also want to emphasize I was making a general comment and not intending a personal criticism.
The points raised by bigiain and mxcrossb are well-made, "cold-like" symptoms are COVID symptoms, the loss of taste and smell only occurs in some cases. CDC has a full list of coronavirus symptoms[1].
I fear that many are flying, socializing etc. when they are actually symptomatic (e.g. headache, sore throat) because they consider these minor symptoms, or perhaps they can just "hope for the best", but the severity of the symptom doesn't change whether or not someone is symptomatic.
The heck is the point of a test if not to confirm or rule out covid? He took two tests, came back negative and assumed his "cold or covid" symptoms were cold until he had reason to believe they were covid. Other than the tests sucking everything in the fact pattern is perfectly reasonable.
Any test has a certain percentage of false positives and false negatives -- in fact, you can likely tune your ratio of false positives to false negatives depending on what your priority is. On a community level, the statistics from testing are essential for monitoring the spread of a disease, but on an individual level a test can still give an incorrect result, so shouldn't be the only factor when making decisions.
For an individual, if they have a negative test AND no symptoms AND no contacts with known COVID-positive individuals, then they can proceed as-if they don't have COVID and take standard precautions. However, if they do have symptoms, then that might mean further testing is required.
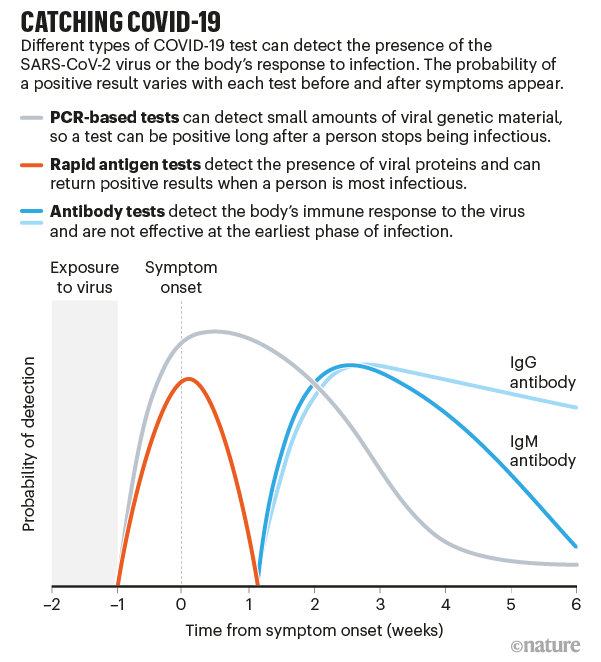
For anyone interested about testing, this graphic is essential:
It shows the difference in test efficacy for different tests (rapid antigen, PCR, antibody tests) as a function of time from symptom onset.
Rapid antigen tests only have a narrow window of efficacy. If they come back positive, you likely have COVID, but if they come back negative you could still have COVID and could still be contagious.
This is also why many countries are requiring PCR tests prior to entry, because they are more effective than rapid antigen tests, although can also give false negatives, especially early after exposure.
In my opinion, the rapid test's greatest value is using it to screen asymptomatic people in a regular (daily or weekly) process. For example, a school would test a random sample of students each day. This could help catch any stealthy clusters. It's not perfect, but it's better than just looking for symptoms.
It's also subtle in that while false negatives are common, false positives are rare (very rare). But general public don't get that subtlty and assume "the test isn't reliable" so a positive means they're not infected.
Almost no tests in existence can confirm or deny particular infection.
Think of them (and symptoms) more as odds updater. If you have 20 minutes to spare this video [0] by 3 Blue 1 Brown is a brilliant introduction to the concept.
{kind=link}
> the assumption I had a minor cold > the loss of smell was total
Since there does seem to be a messaging problem about the reliability of testing, I think it's worth emphasizing: if someone has symptoms of COVID, they should proceed as-if they have COVID. CDC guidance[1] is to isolate if you have a positive test OR if you have symptoms.
To do otherwise is to gamble with the health and lives of the people they meet, and the people those people meet, and so on. It may prove almost impossible to show who caught COVID from whom, but that doesn't mean that ignoring guidance won't lead to deaths. A statistical death is still the death of a real person, even if we can't put a name to them.
[1] https://www.cdc.gov/coronavirus/2019-ncov/if-you-are-sick/is...